2025 Outcomes Report (Dr. Warner)
One of the core values of our service is measurement and transparency. Thus, every year we review all surgical cases performed by physicians on our service and report these publicly for prospective and current patients to review as they wish. This is a short-term review as we perform longer-term analysis for publication and for cohort reporting for all patients separate from this report. By measuring outcomes, we can analyze our treatment in order to continually improve care.
Dr. Warner’s outcomes data is collected and compiled by the clinical research coordinator for the service, utilizing the electronic medical records system of Massachusetts General Hospital as well as surgical billing data. Our methodology consists of a review of all operations performed during the calendar year on a case-by-case basis, with special consideration made to procedure type, patient past surgical history (primary vs. revision status), and any complications arising during or after an operation. This data was collected, aggregated, and independently analyzed by the research coordinator with no direct input from the attending physician. The final review was performed by the surgeon in order to check accuracy of procedures and outcomes.
2025 Surgical Overview
The following section will provide an overview of all cases done by Dr. Warner in 2025. Importantly, procedures are not the same as total surgeries performed – one surgery may (and often does) include multiple procedures completed during the same operation. For example, a patient may undergo a shoulder arthroplasty and a biceps tendon tenodesis during the same surgery. These are recorded below as separate procedures, but as a single surgery.
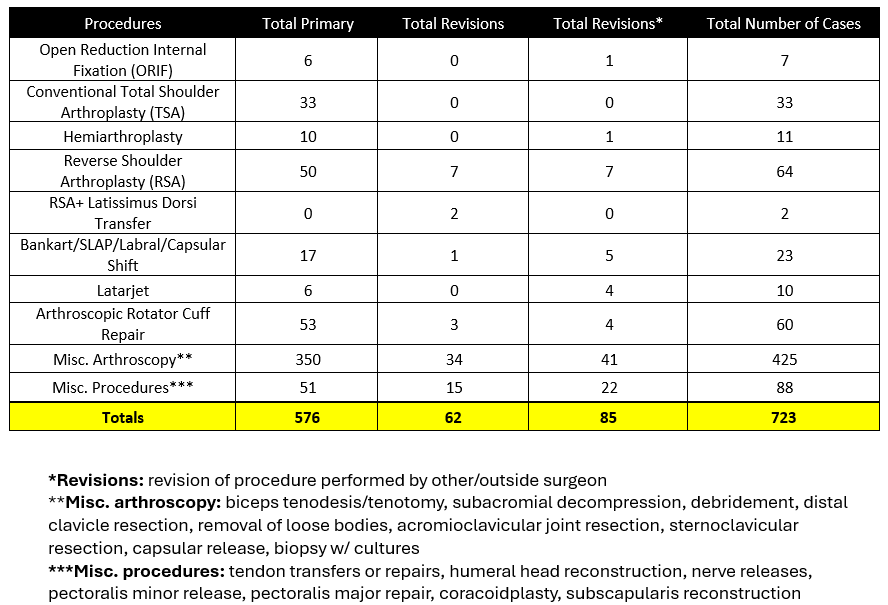
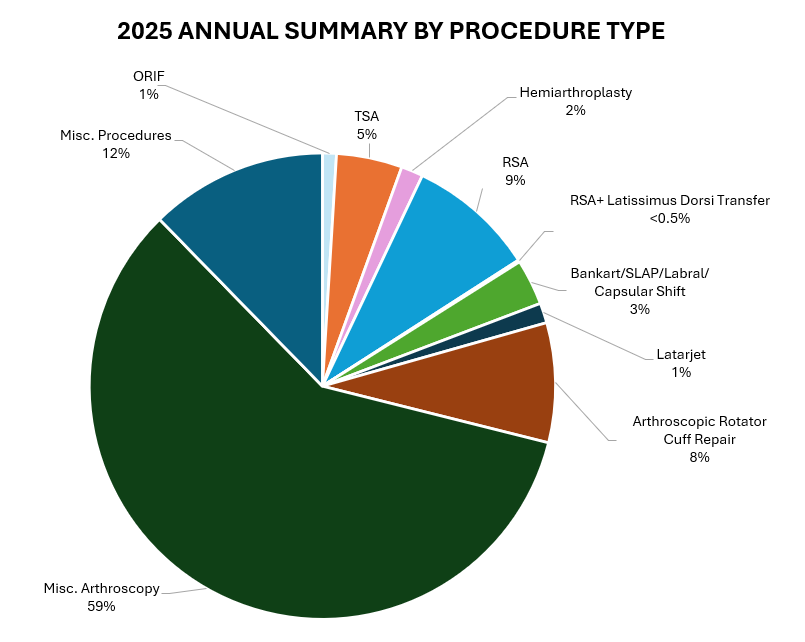
- 723 procedures were performed on 273 patients by Dr. Warner during the 2025 calendar year across.
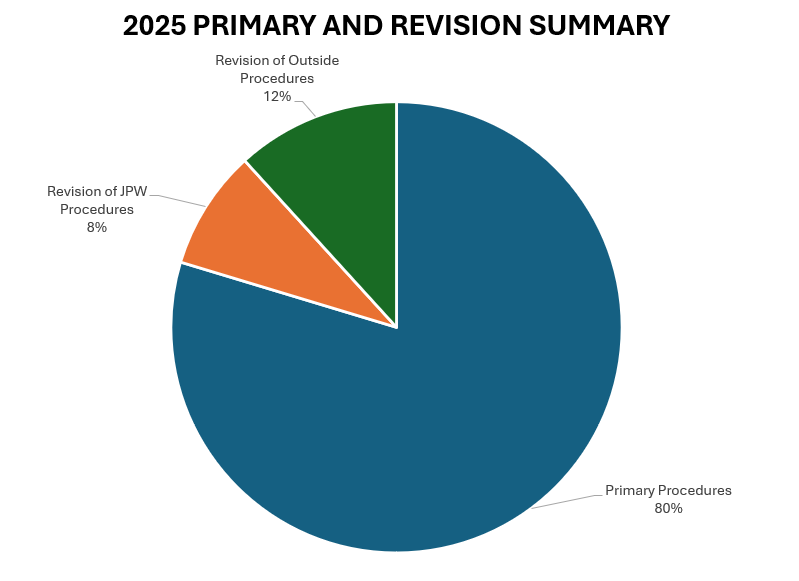
- Of these 723 procedures, 576 were primary procedures. A “primary” procedure refers to the first surgical intervention done for a patient’s condition. If Dr. Warner performs a rotator cuff repair on a patient who has not had a repair done on that shoulder yet, this would be considered a primary surgery. 62 of these procedures (29 patients) were revisions of his own past cases (these revisions were performed in 2024, but the primary procedure was done at a prior time time). 85 of these procedures (34 patients) were revisions of procedures performed by other/outside surgeons.
2025 Revision Descriptions
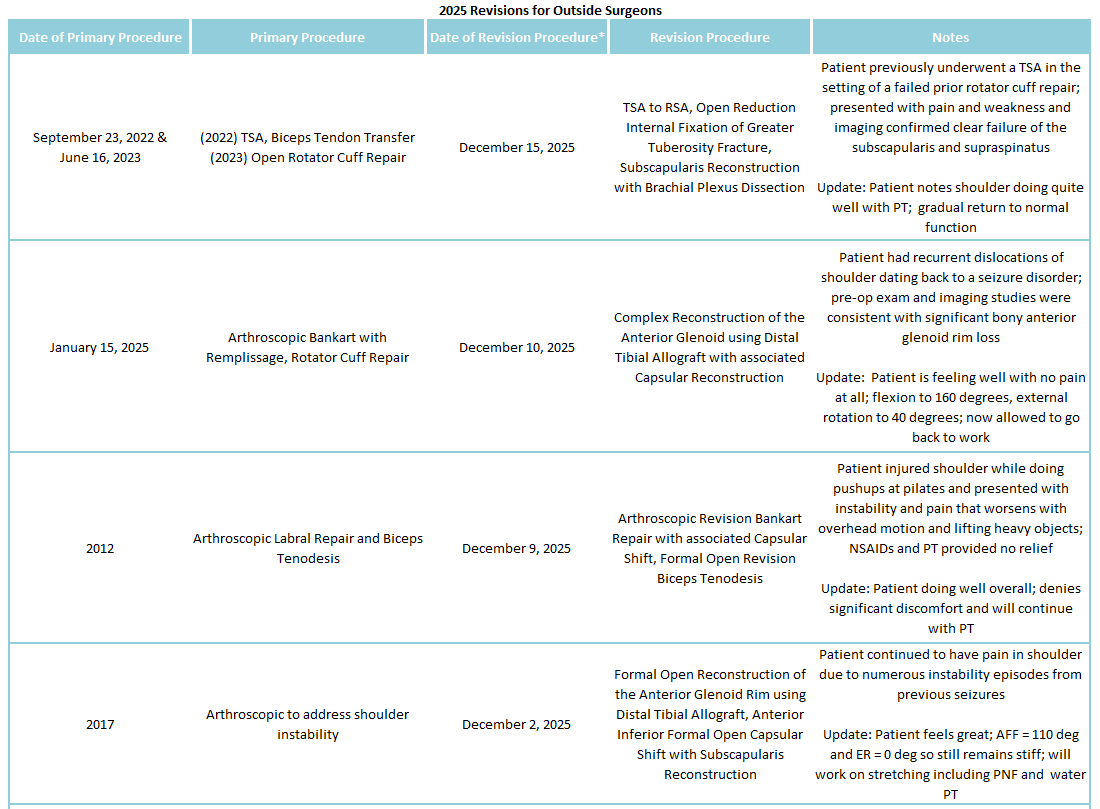
Of the 9% of Dr. Warner’s 2025 cases that were revisions, the average interval between primary and revision surgery was about 6.02 years. The shortest interval was 120 days, and the longest interval was 314 months or about 26 years. These revision procedures are summarized below:
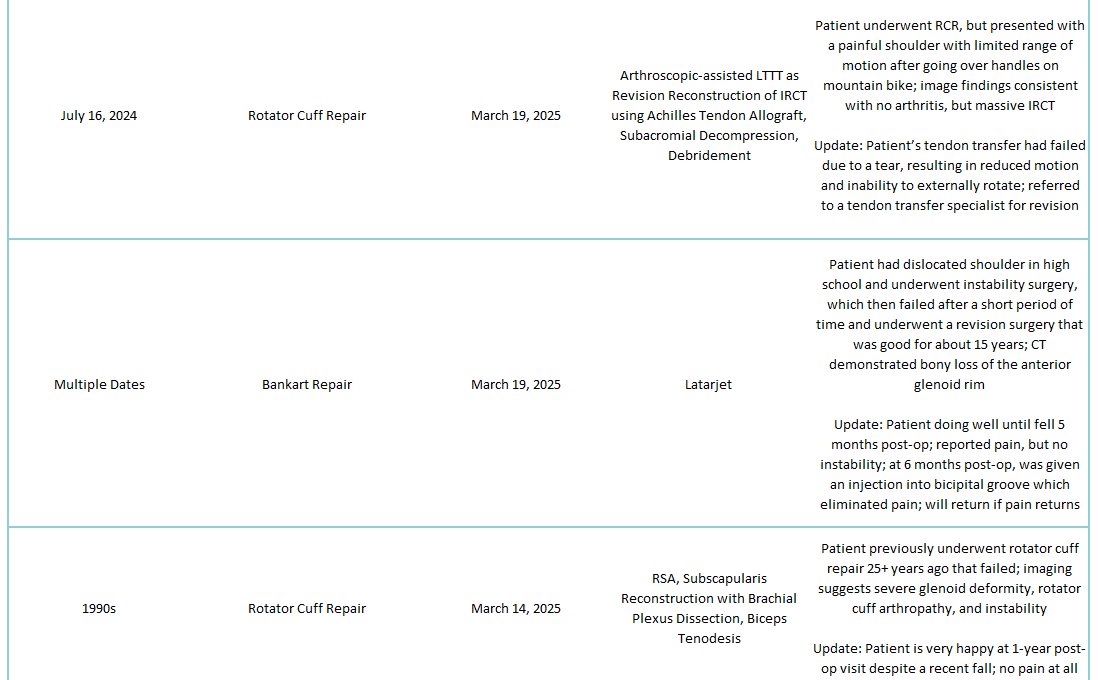
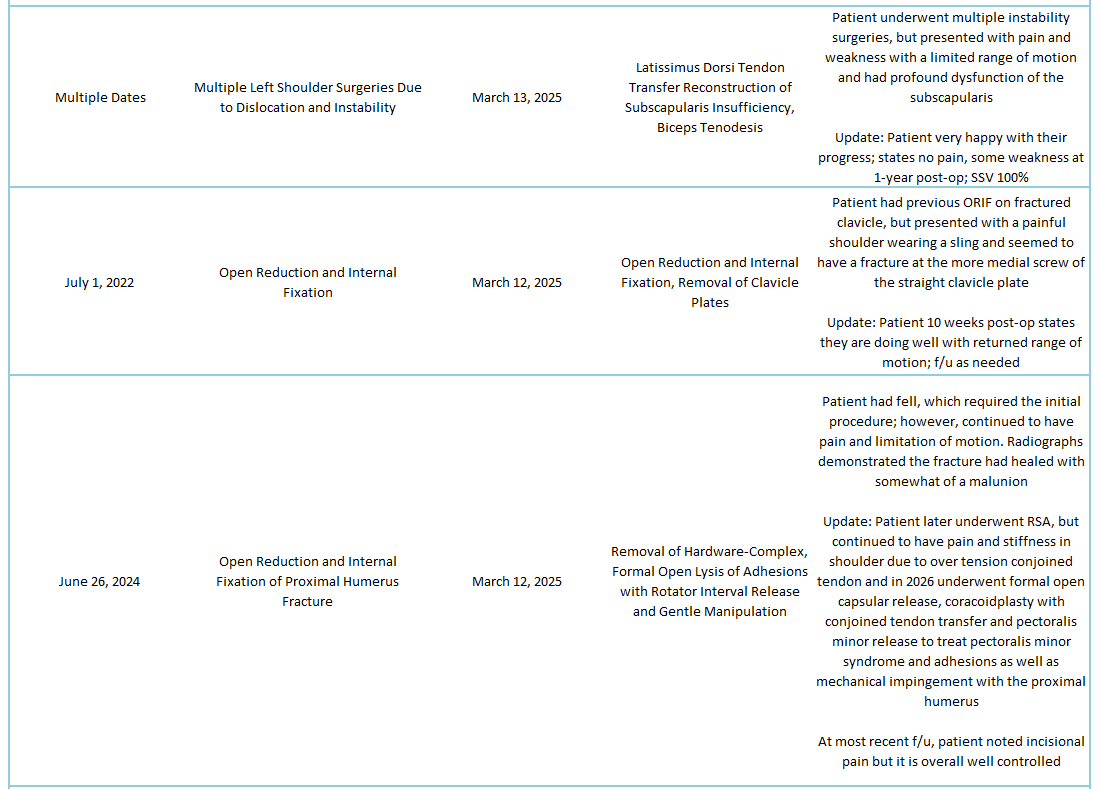
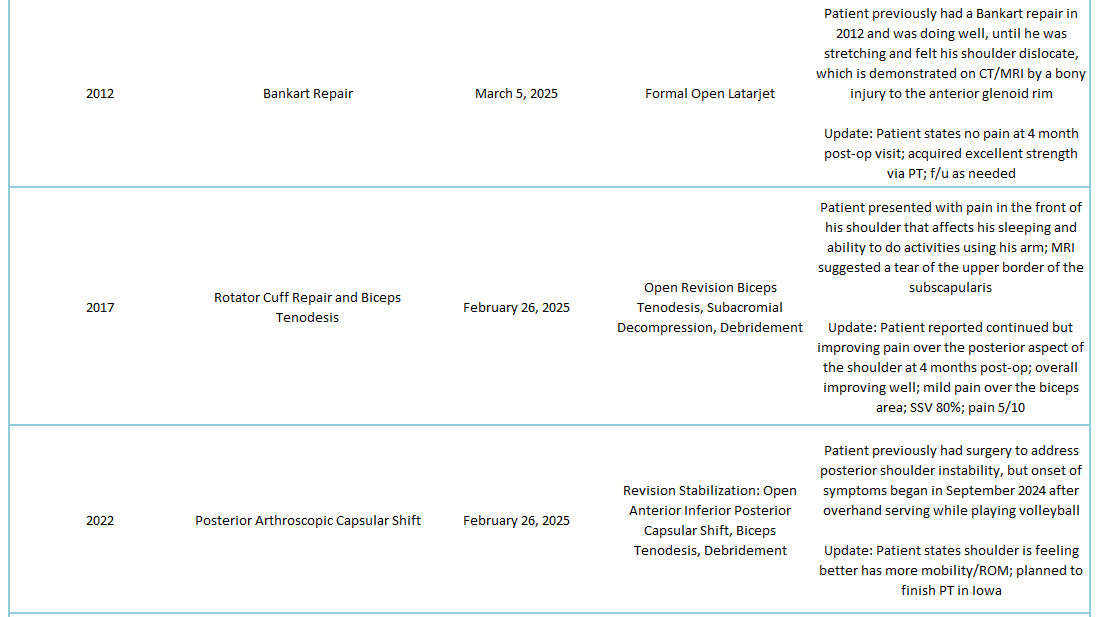
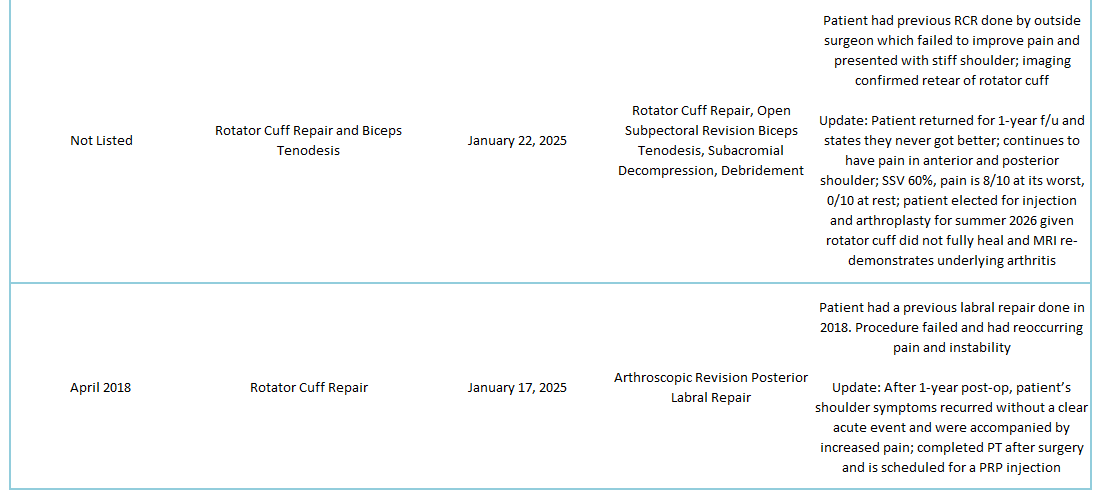
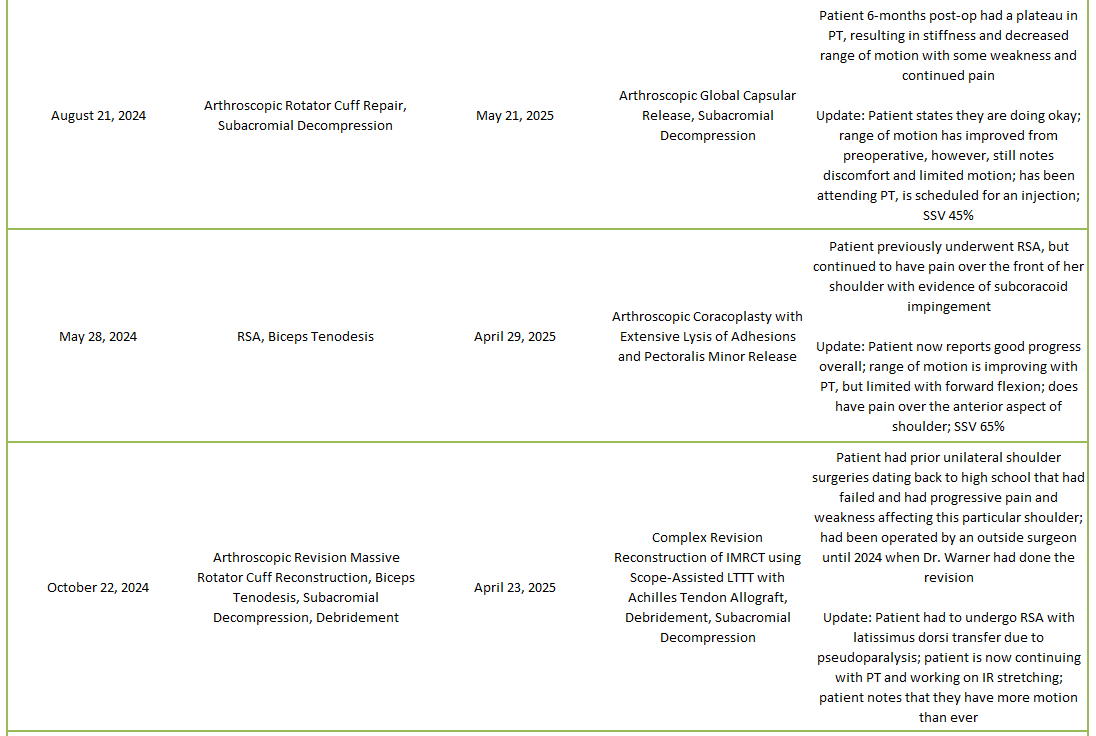
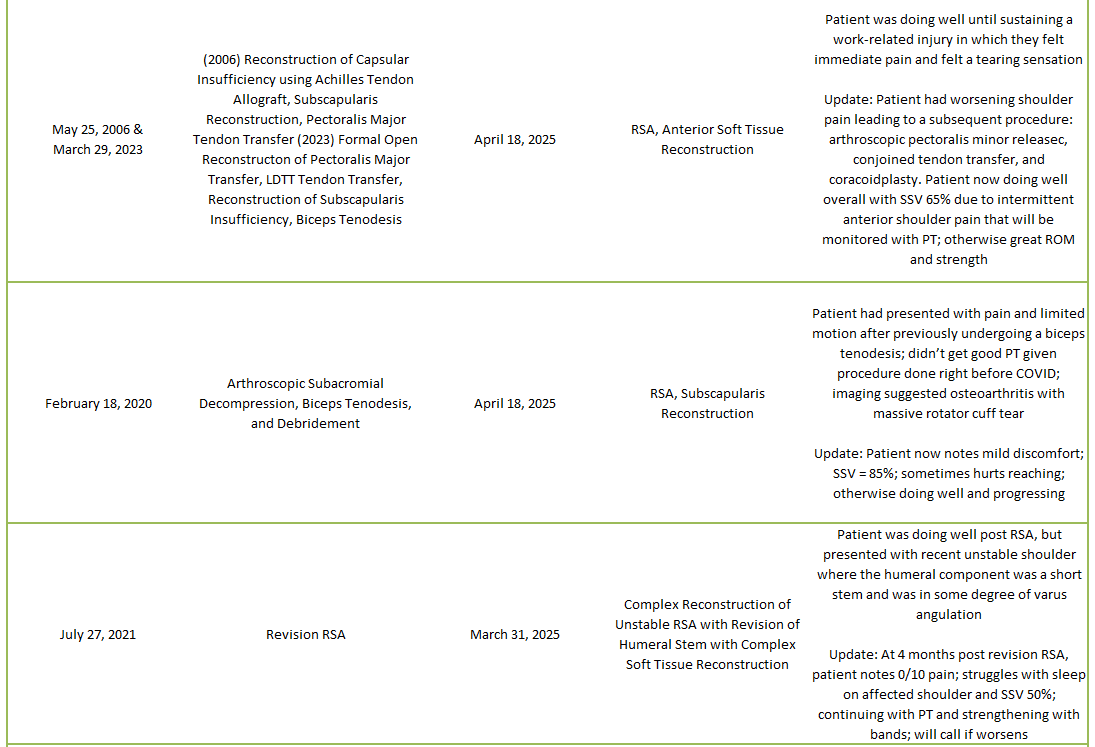
2025 Revisions (Outside Cases)
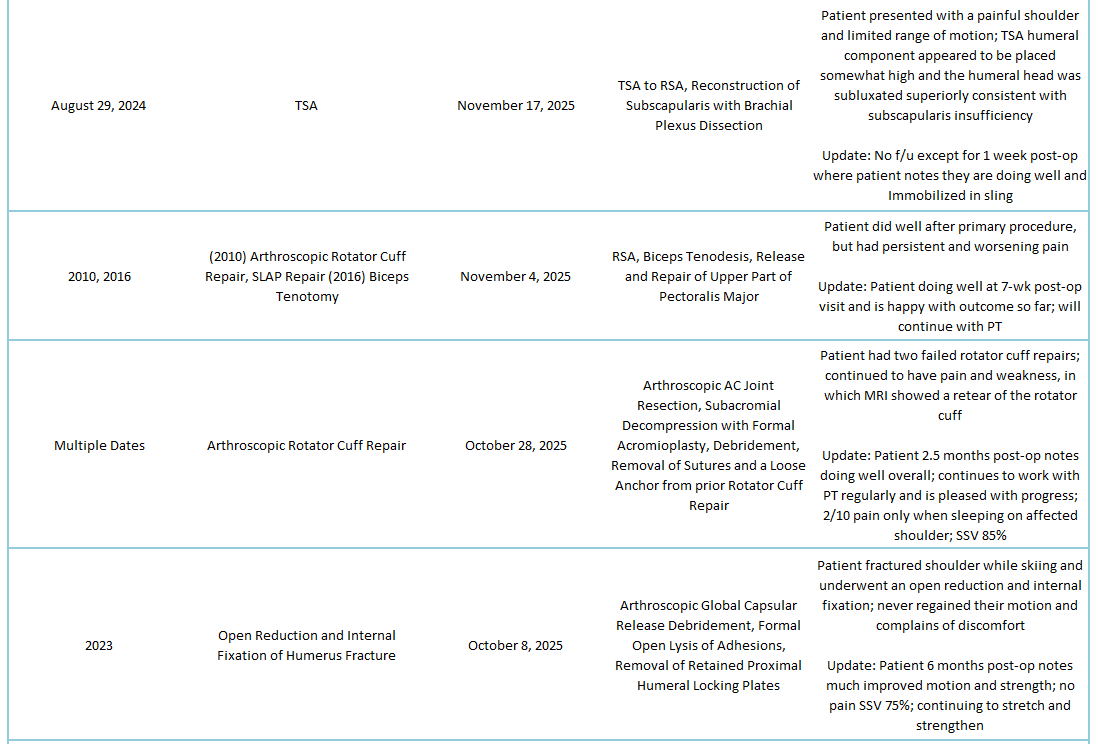

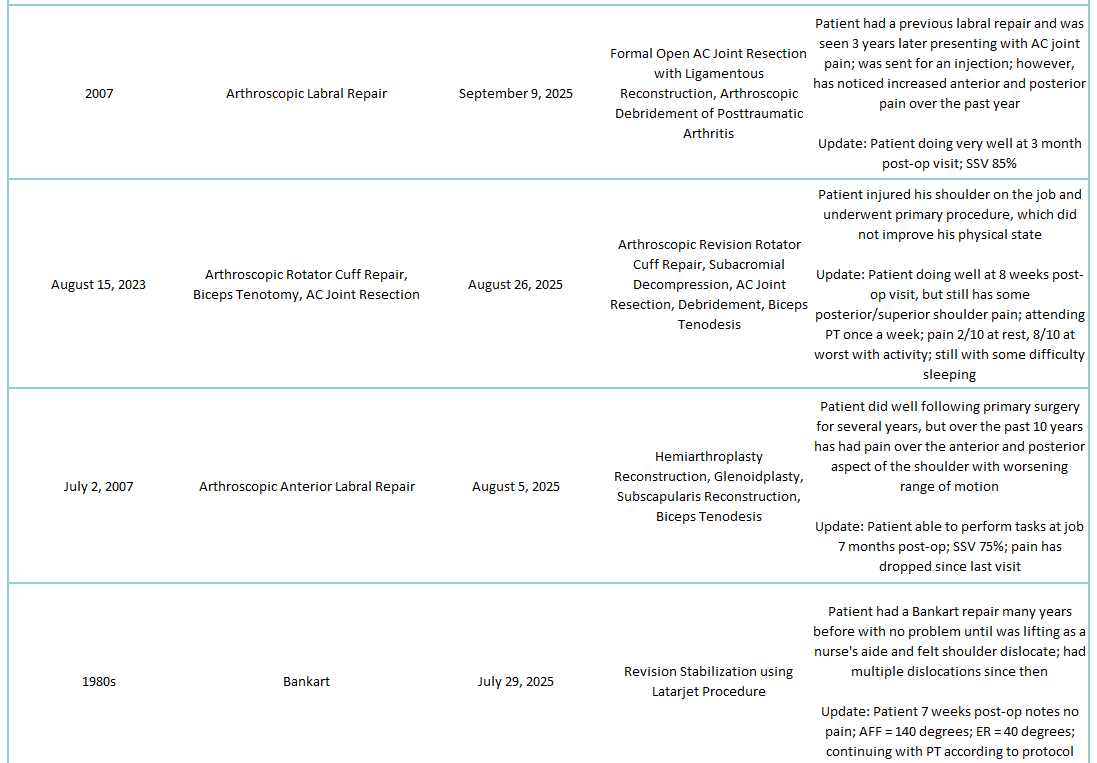
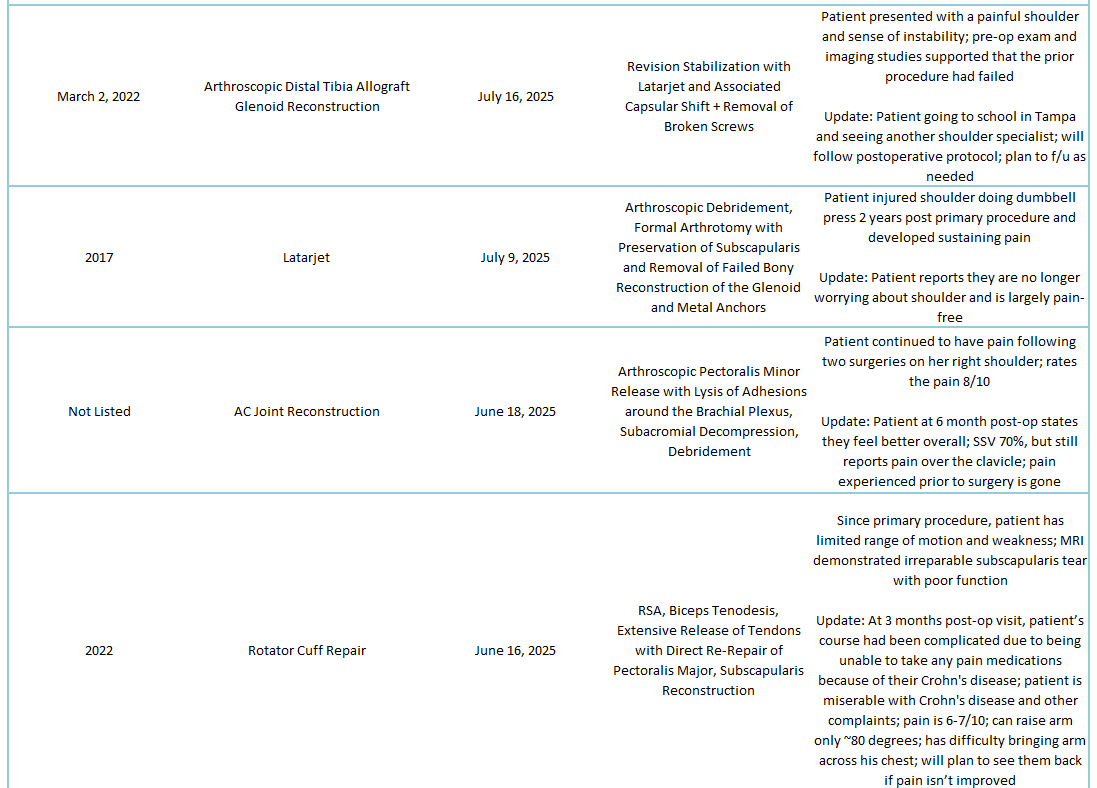
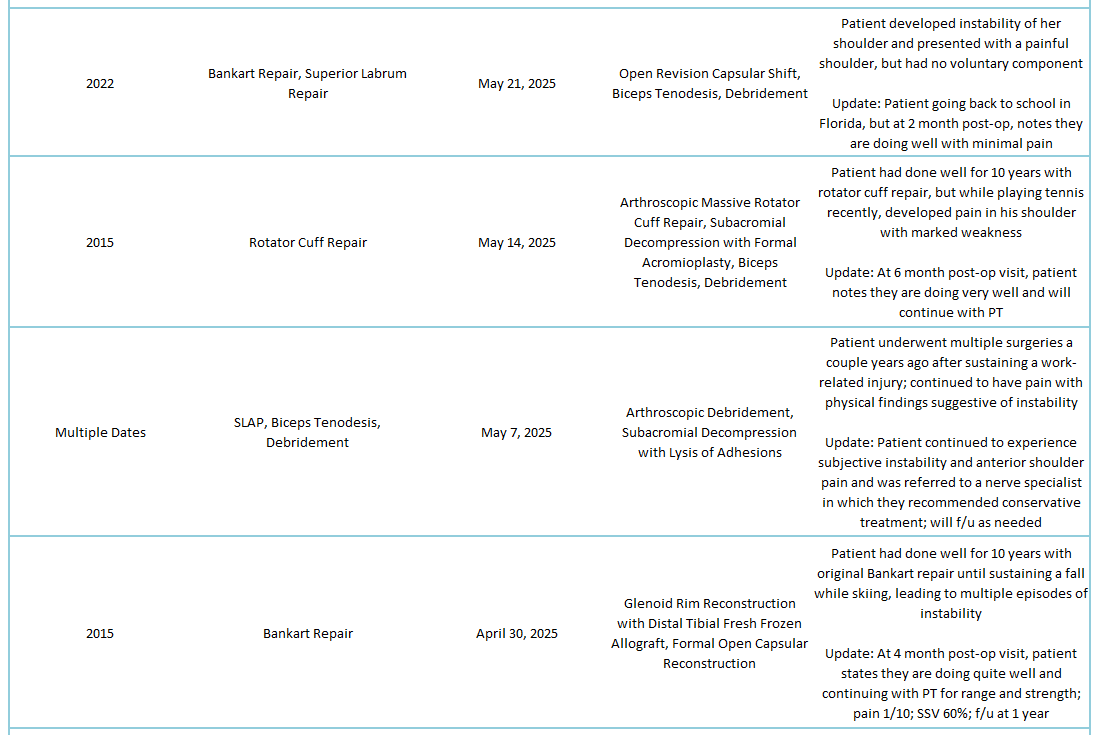
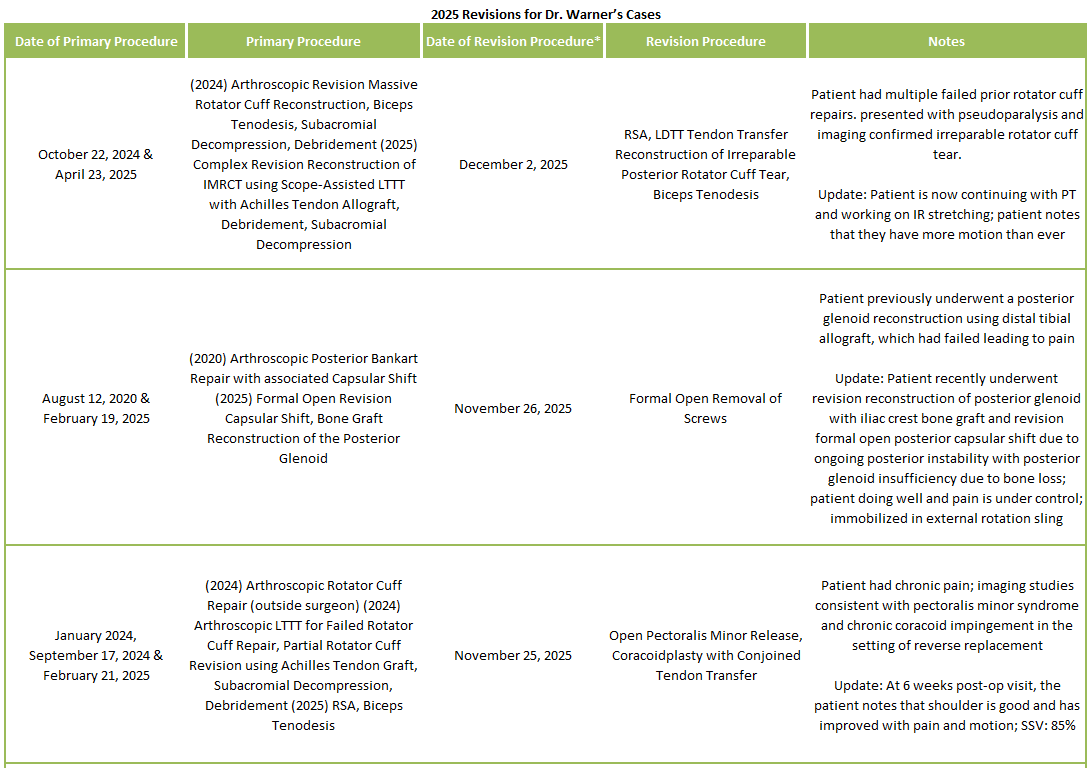
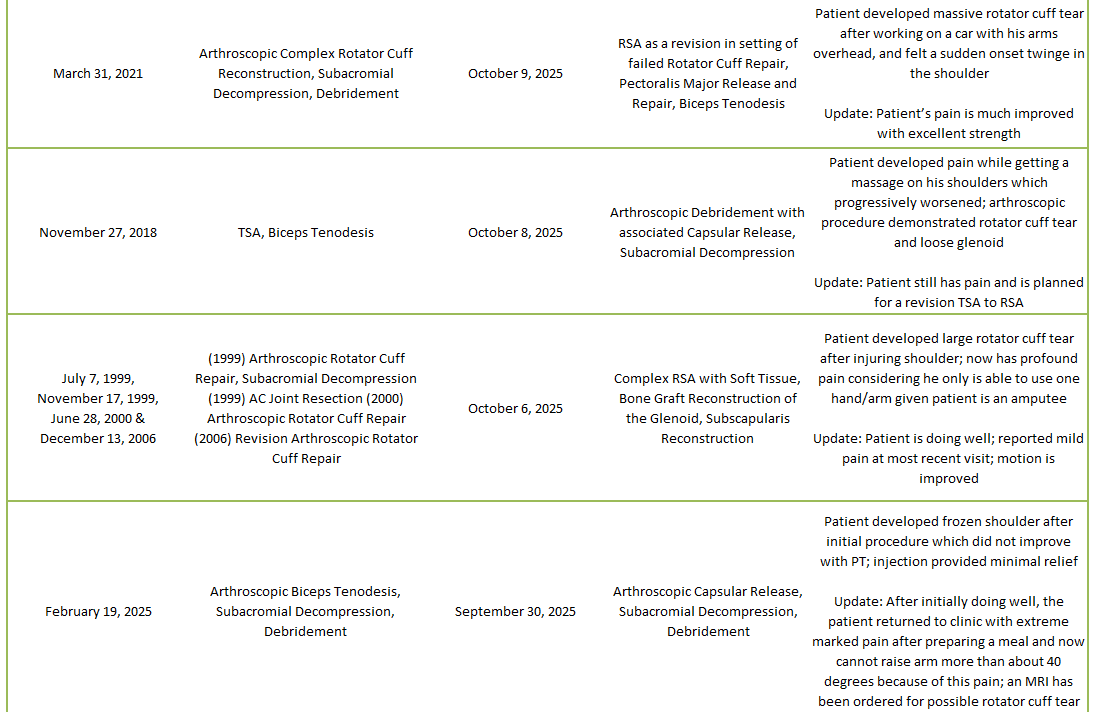
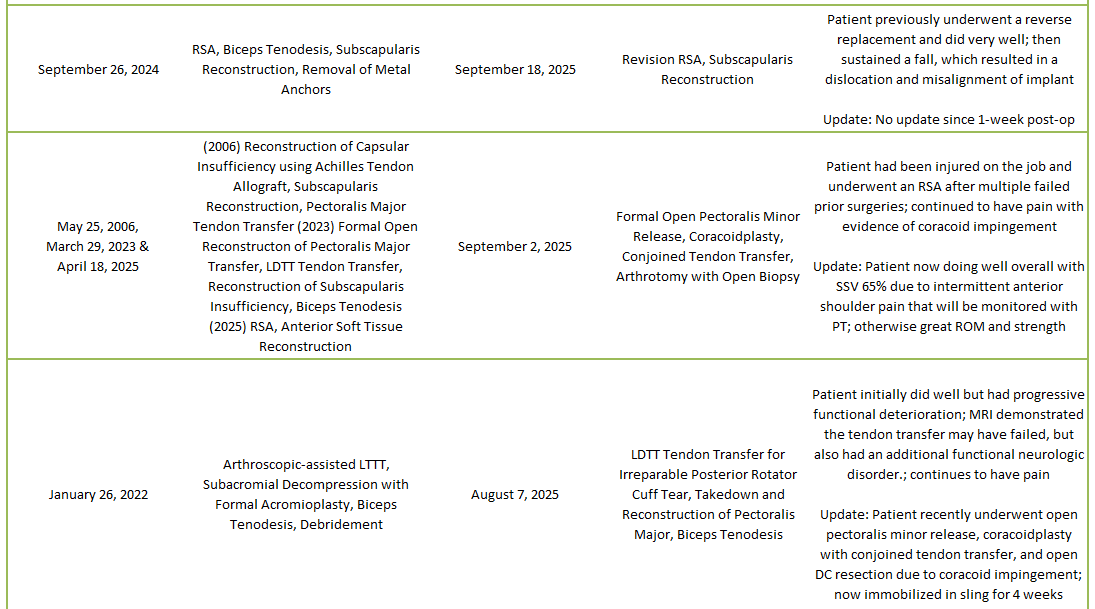
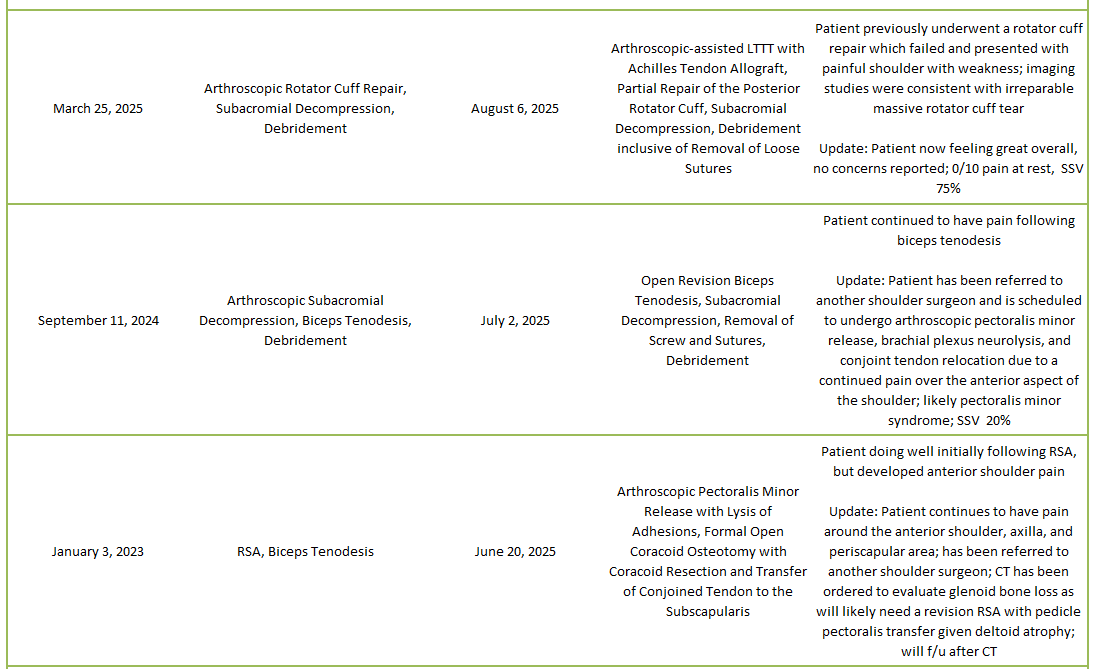
2025 Revisions (Dr. Warner’s Cases)



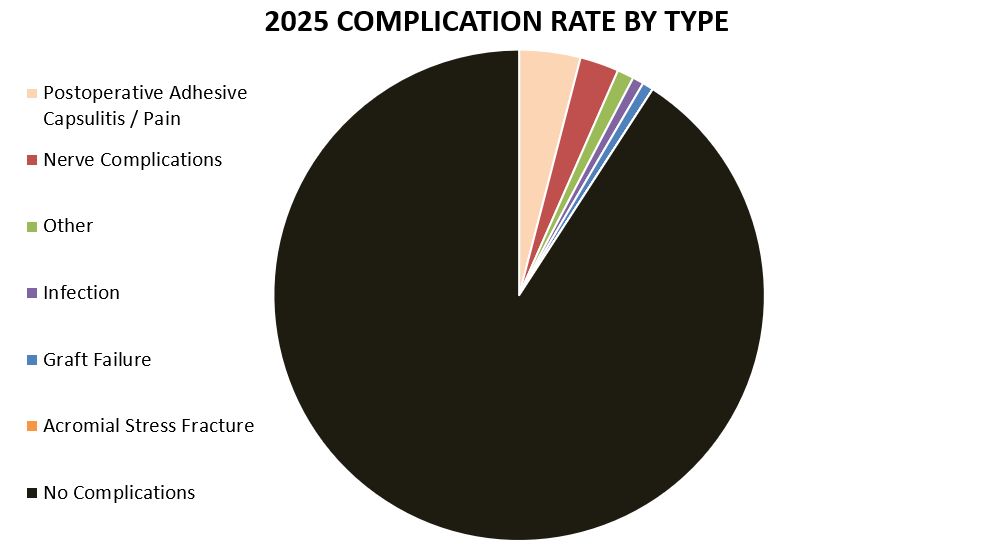
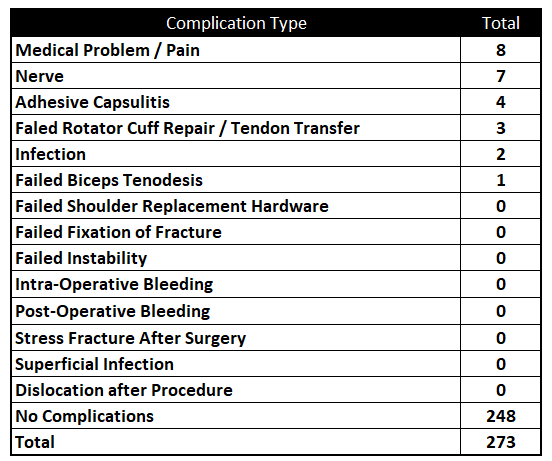
2025 Complications Overview
Of 273 patients operated on by Dr. Warner in 2025, 25 patients (9.1%) experienced a complication during or after surgery. These complications were identified in 2025. Of the 25 complications, 7 required additional surgeries, 2 have upcoming planned surgeries, while the overall re-operation rate was 2.6% (11 reoperations out of 273). An explanation of each complication can be found below. Descriptions in green were patients who had resolution of their complication and those indicated in red have an ongoing issue at the time of this reporting.
Postoperative Adhesive Capsulitis / Pain
This patient underwent a removal of hardware by Dr. Warner after having had a proximal humerus open reduction internal fixation done by another surgeon. Following the removal, patient reported no improvement in pain or motion after completing 6 weeks of home therapy. Patient then underwent reverse shoulder arthroplasty after removal of hardware due to pain, stiffness, and evidence of avascular necrosis, which did not improve function as post-op course was complicated by significant pain that interfered with ability to do any physical therapy or even drive. The patient does have fibromyalgia and recently underwent formal open capsular release, coracoidplasty with conjoined tendon transfer and pectoralis minor release to treat pectoralis minor syndrome and adhesions as well as mechanical impingement with the proximal humerus in 2026. At most recent follow-up, patient noted incisional pain, but it is overall well controlled.
This patient underwent an arthroscopic capsular release and developed stiffness following surgery with worsening symptoms than prior to surgery. The patient was given a fluoroscopic-guided injection of cortisone into the glenohumeral joint and the subacromial space which should allow to return doing physical therapy and improve. Will follow-up as needed.
This patient underwent an arthroscopic biceps tenodesis and developed stiffness and frozen shoulder following surgery. The patient is working with physical therapy to improve.
This patient underwent an arthroscopic global capsular release and subacromial decompression in the setting of frozen shoulder and type II diabetes which healed, however the patient developed anterior pain. The patient notes improvement in shoulder pain, but is unable to perform therapy due to the pain in the rest of his arm. Patient has tried a wrist brace, elbow brace, and elbow compression sleeve which have not been effective. Patient will see a nerve and elbow specialist for possible treatment.
This patient underwent a reverse shoulder arthroplasty and remains in pain 3 months post-op. The patient’s course has been complicated by the fact that they cannot take any pain medications because of their Crohn’s disease. The patient will follow up if pain has not improved significantly and will discuss pain management with other providers doctors to be given therapy input.
This patient underwent an arthroscopic debridement and continued to have subjective instability and pain principally with flexion. After four shoulder surgeries, the patient feels as if their symptoms have not been resolved and feels a catching sensation in the front of the shoulder. Patient is getting treated conservatively from a nerve specialist who provided a Botox injection into the pectoralis minor as well as shoulder pacemaker.
This patient underwent an arthroscopic suprascapular nerve release and decompression and developed increased pain and loss of motion, consistent with adhesive capsulitis evolving after surgery. The patient received a fluoroscopic-guided injection into the glenohumeral joint to alleviate symptoms and proceed with physical therapy.
This patient underwent a reverse shoulder arthroplasty following failed prior failed rotator cuff surgeries and developed pain two weeks post-surgery. Patient underwent a following procedure of open pectoralis minor release and conjoined tendon transfer. Patient now doing well overall with SSV 65% due to intermittent anterior shoulder pain that will be monitored with PT; otherwise great ROM and strength.
Patient underwent an arthroscopic subacromial decompression and open revision biceps tenodesis and reported posterior shoulder pain after shoulder and mild pain over biceps area. Physical therapy has improved the posterior shoulder pain, although patient notes a dull ache in his biceps region that he feels intermittently, but overall improving well.
This patient underwent an arthroscopic biceps tenodesis and subacromial decompression and developed postoperative frozen shoulder. The patient was sent for an intra-articular corticosteroid injection which provided them with significant relief. However, the patient later underwent revision arthroscopic capsular release and subacromial decompression with debridement for frozen shoulder. After initially doing well, the patient returned to clinic with extreme marked pain after preparing a meal and now cannot raise arm more than about 40 degrees because of this pain; an MRI has been ordered for possible rotator cuff tear.
This patient underwent a rotator cuff repair and open subpectoral revision biceps tenodesis one year ago, and states that shoulder never felt quite right after surgery. The patient continues to have anterior and posterior shoulder as the rotator cuff has not fully healed when returned for 1-year follow-up. Patient has underlying arthritis and rotator cuff healing likely relevant to her age. Patient elected for injection at visit and will schedule shoulder arthroplasty for summer 2026.
Nerve Complications
This patient developed swelling and hand and finger tingling immediately after reverse shoulder arthroplasty surgery. The patient has seen another orthopedist in which their exam was consistent with the diagnosis of carpal tunnel syndrome. The patient is continuing with physical therapy. Patient’s shoulder is now feeling well with a decrease in pain. Patient will continue with PT on her own.
This patient underwent a total shoulder arthroplasty and began to experience ulnar nerve pain within the medial aspect of the elbow radiating into the pinky and ring finger, characterized by numbness and tingling a week post-op. The nerve was found to be mobile and inflamed post-surgery. Patient is planning to continue with physical therapy and if more bothersome they will arrange for another evaluation. Patient saw an outside physician and said patient had nerve irritation. They suggested an EMG study and provided the patient a Medrol dose pack.
This patient underwent a reverse shoulder arthroplasty and reported not much pain in shoulder, but has likely developed Parsonage-Turner syndrome, which has been improving. The patient also developed a pulmonary embolism following surgery which has been treated with Eliquis. At a recent follow-up visit, the patient states they are very happy with the procedure as pain level varies from 0 to 3 on a 0 to 10 scale. Most recent EMG describes that they have a median nerve problem around the elbow, but also carpal tunnel syndrome, so will continue to monitor with the hand specialists.
This patient underwent an arthroscopic Bankart repair following a traumatic head and shoulder injury as the result of a fall while ice skating. The patient remained weak after her surgery. This patient had to stop working due to poor function and an EMG demonstrated mild axillary nerve dysfunction. Patient has been referred to a nerve specialist who diagnosed the patient with a scapular motion problem and recommended conservative management consisting of pectoralis minor Botox injection, shoulder pacemaker for the neuroplasticity, and sports psychotherapy. Her most recent exam showed improvement from STAM type IIb to STAM type IIa and has been advised to continue the same measures that they have been doing now. Has returned to work part-time and will be re-evaluated in 2 months.
This patient underwent a reverse shoulder arthroplasty and presented with hand/wrist pain which began without injury following surgery. The patient reports almost no shoulder, however, having complaints of numbness/tingling occurring along ulnar side three digits, localized pain to the region of the dorsal hand/wrist joint, and clicking. The patient underwent carpal and cubital tunnel release for carpal and cubital tunnel syndrome by another surgeon and is now doing well overall. Pain is minimal/well controlled.
This patient underwent an arthroscopic capsular release and sought out a hand specialist after developing numbness and tingling in the fingers and in the superficial radial nerve distribution that had been present since surgery. The patient continues to complain of some discomfort in her shoulder, but admits has not been doing much therapy recently, but is going to continue with therapy and aqua therapy.
This patient underwent an arthroscopic rotator cuff repair one year ago. They have noted numbness and decreased function of the right hand, specifically within the distribution of the median nerve at the level of the wrist to the distal first 3 digits after surgery. They have seen a hand specialist who has diagnosed median nerve compression just above the elbow and has offered her a decompression of the nerve. They have been taking gabapentin for the pain and is unable to lay on her affected side. Their hand function has improved is considering if they are ready to proceed with median nerve decompression at the elbow area; shoulder is not a problem.
Infection
This patient underwent a reverse shoulder arthroplasty and developed a surgical site infection. Patient required a subsequent irrigation and debridement procedure by another physician within the Shoulder Service team. Patient is doing fair overall and has been discharged from physical therapy.
This patient underwent a formal open capsular release after multiple shoulder surgeries. The patient was doing well until complaints of a worsening dull ache in the shoulder over several years and made worse by movement. One culture collected at time of surgery grew moderate bacillus species and was treated with trimethoprim-sulfamethoxazole.
Graft Failure
This patient underwent a latissimus dorsi tendon transfer after a previous failed lower trapezius tendon transfer and lost his ability to externally rotate due to the ruptured graft. The patient recently underwent open pectoralis minor release, coracoidplasty with conjoined tendon transfer, and open DC resection due to coracoid impingement; now immobilized in sling for 4 weeks.
This patient underwent a lower trapezius tendon transfer, which was their fourth surgery, and presented with a failed lower trapezius tendon and pseudoparalysis. The patient then underwent a reverse shoulder arthroplasty and latissimus dorsi tendon transfer and is now continuing with PT and working on IR stretching; patient notes that they have more motion than ever.
Other
This patient underwent a distal tibial allograft reconstruction of glenoid and reports stiffness in their shoulder. The patient’s postoperative course was complicated by a pulmonary embolism following surgery, but is now continuing with physical therapy. At a recent follow-up, patient stated they had minimal pain.
This patient underwent a surgery to revise a failed biceps tenodesis performed more than a year ago. After surgery he had pain that he described as burning over the front of his shoulder. The patient is seeing saw a nerve specialist who diagnosed a rare condition known as Pectoralis Minor Syndrome. This seemed to be unrelated to the surgery as it was not near the area operated. They received an injection into the affected area that gave him some relief. However, at a recent follow-up, patient continues to struggle with pain over the anterior aspect of the shoulder; reports pain on average 7/10, and SSV of 20%. Is now scheduled for surgery.
This patient underwent an arthroscopic rotator cuff repair which failed due to the patient pushing up from the floor from a squatted position with their weight on the affected shoulder and felt a tearing sensation. Imaging confirmed rupture and then underwent an arthroscopic lower trapezius tendon transfer and partial repair of the rotator cuff. Patient now feeling great overall with no concerns reported; 0/10 pain at rest, SSV 75%.