2025 Outcomes Report (Dr. Lohre)
One of the core values of our service is measurement and transparency. Thus, every year we review all surgical cases performed by physicians on our service and report these publicly for prospective and current patients to review as they wish. This is a short-term review as we perform longer-term analysis for publication and for cohort reporting for all patients separate from this report. By measuring outcomes, we are able to analyze our treatment in order to continually improve care.
Dr. Lohre’s outcomes data is collected and complied by the clinical research coordinator for the service, utilizing the electronic medical records system of Massachusetts General Hospital as well as surgical billing data. Our methodology consists of a review of all operations performed during the calendar year on a case-by-case basis, with special consideration made to procedure type, patient past surgical history (primary vs. revision status), and any complications arising during or after an operation. This data was collected, aggregated, and independently analyzed by the research coordinator with no direct input from the attending physician.
2025 Surgical Overview
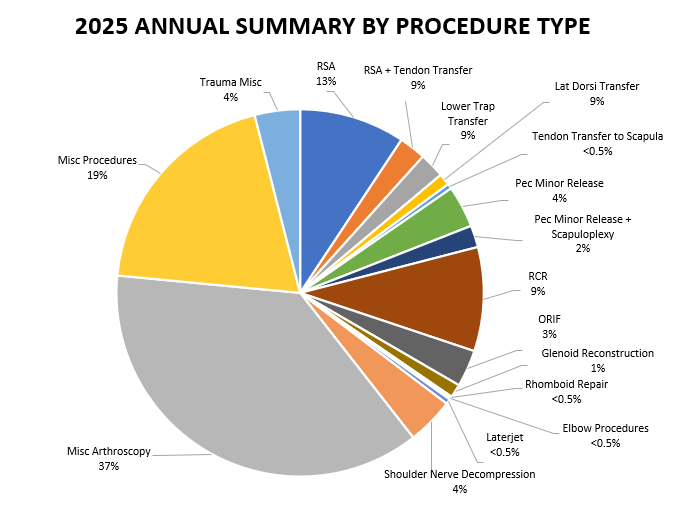
The following section will provide an overview of all cases done by Dr. Lohre in 2025. Importantly, procedures are not the same as total surgeries performed – one surgery may (and often does) include multiple procedures completed during the same operation. For example, a patient may undergo a shoulder arthroplasty and a biceps tendon tenodesis during the same surgery. These are recorded below as separate procedures, but a single surgery. If you have any questions regarding the methodology of data analysis and reporting, please contact Dr. Lohre directly.
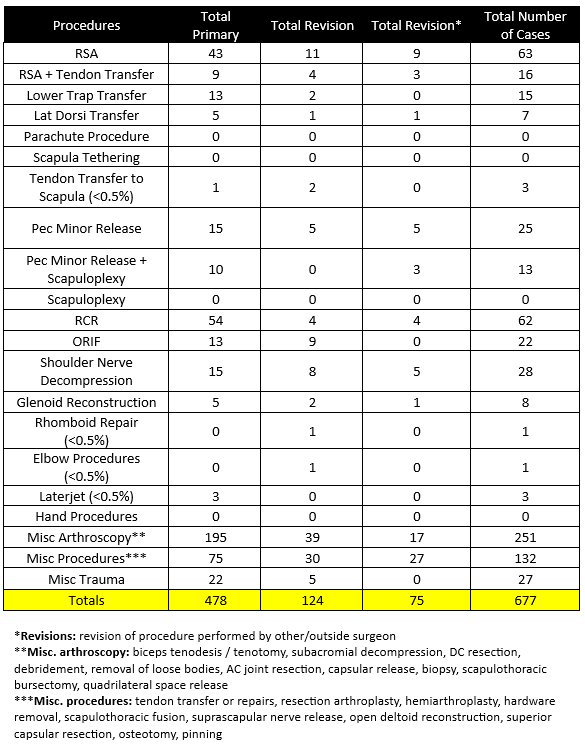
- 677 procedures were performed by Dr. Lohre during the 2025 calendar year across 283 total cases.
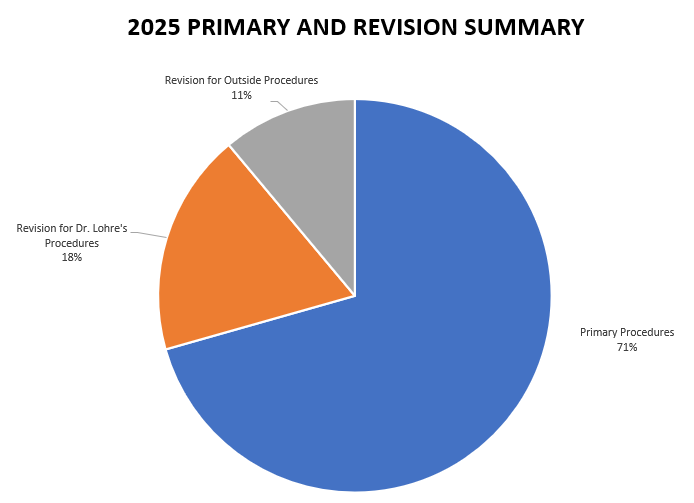
- Of these 677 procedures, 478 were primary procedures. A “primary” procedure refers to the first surgical intervention done for a patient’s condition. If Dr. Lohre performs a rotator cuff repair on a patient who has not had a repair done on that shoulder yet, this would be considered a primary surgery. 124 of these procedures (45 patients) were revisions of his own past cases (these revisions were performed in 2025, but the primary procedure was done at a prior time time). 75 of these procedures (30 patients) were revisions of procedures performed by other/outside surgeons
2025 Revision Descriptions
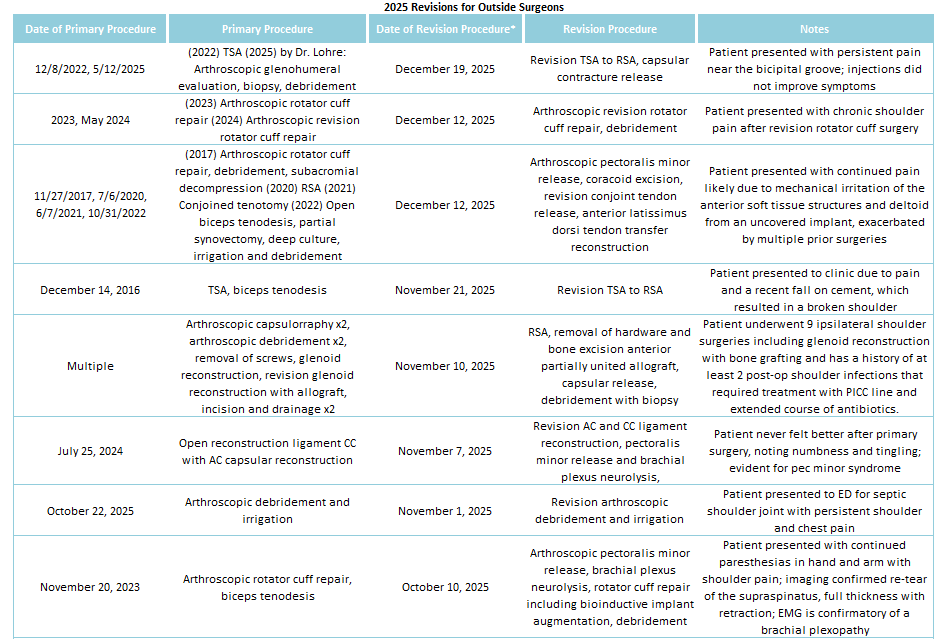
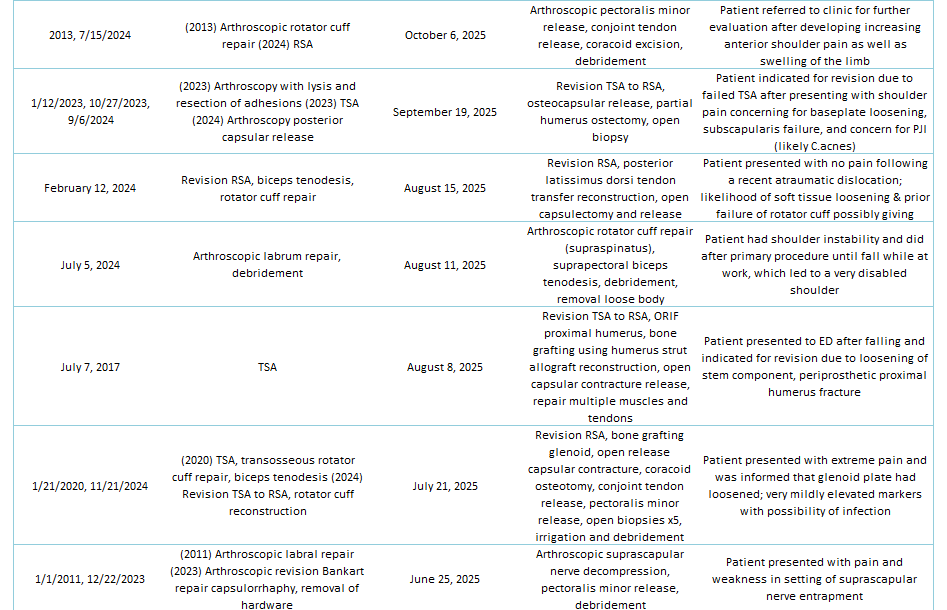
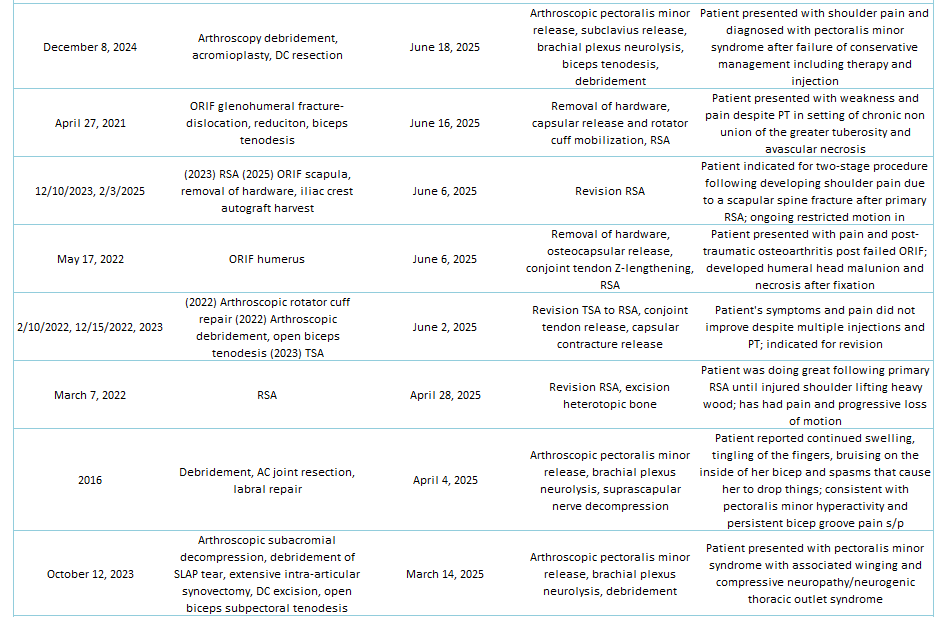
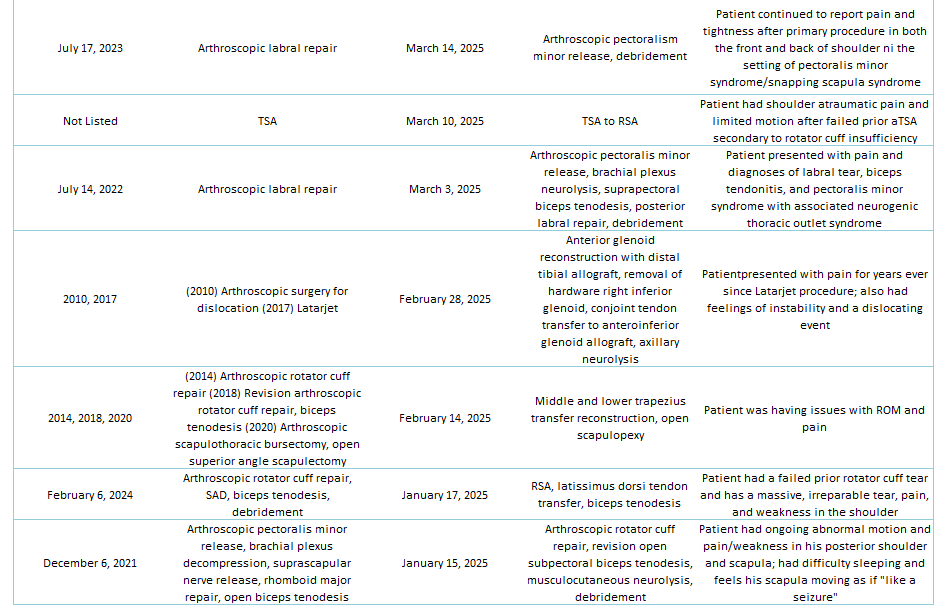
Of the 29% of Dr. Lohre’s 2025 cases that were revisions, the average interval between primary and revision surgery was about 1.5 years. The shortest interval was 9 days, and the longest interval was 108 months or about 9 years. These revision procedures are summarized below:
2025 Revisions (Outside Cases)
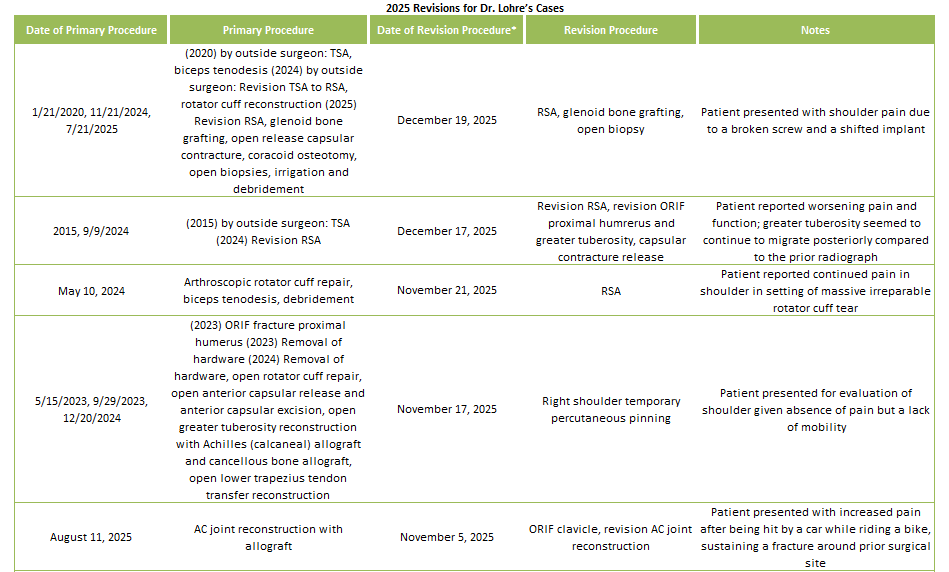
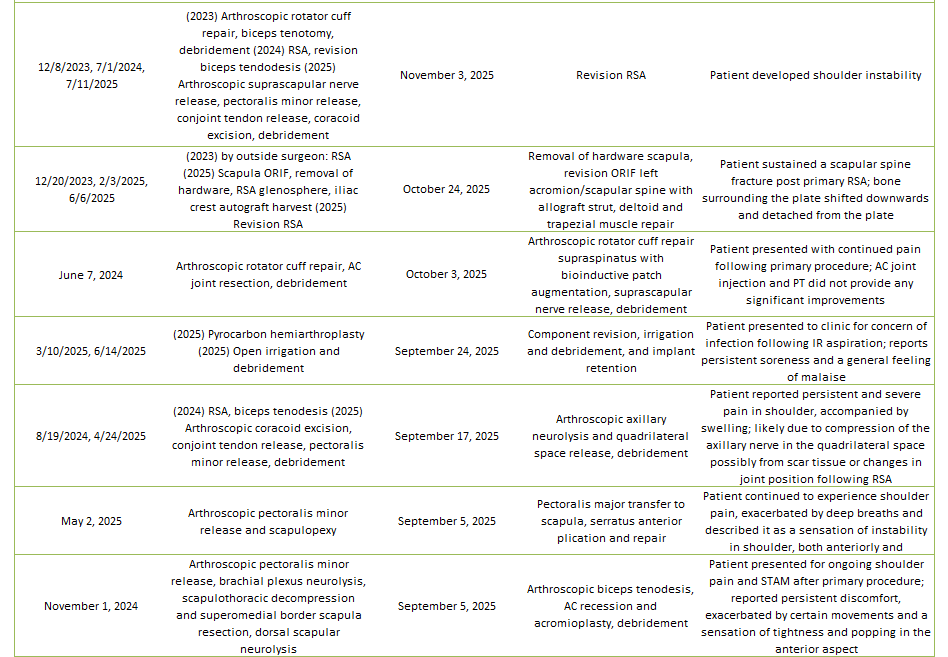
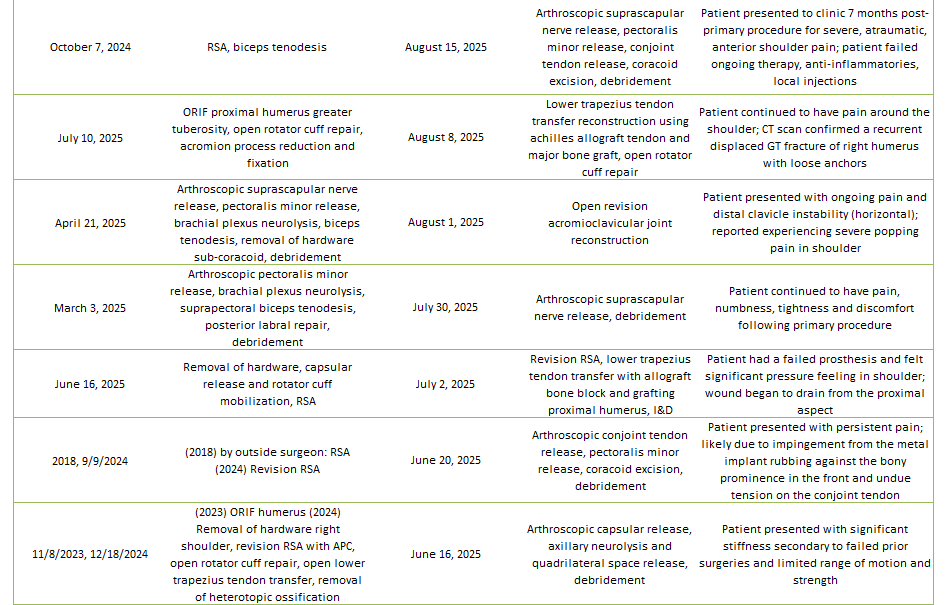
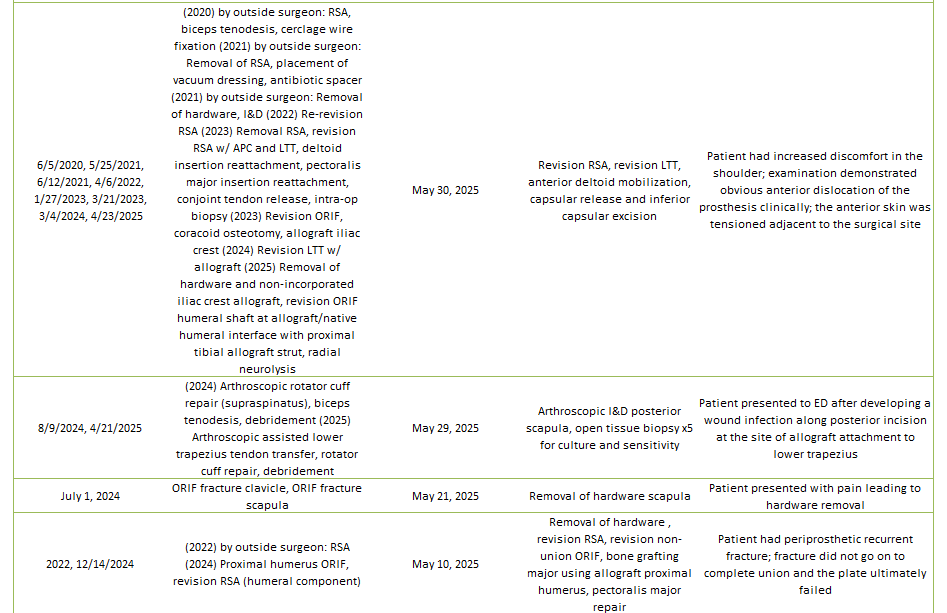
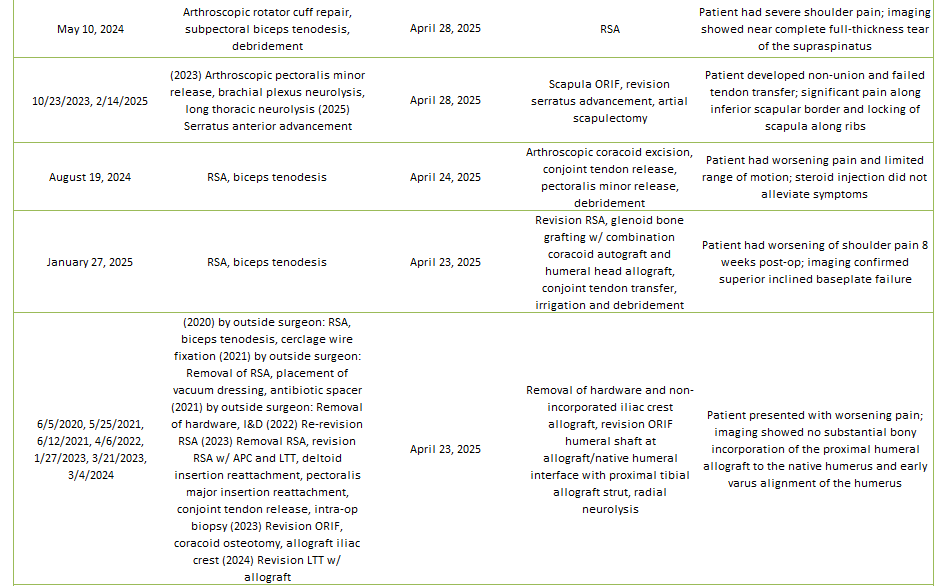
2025 Revisions (Dr. Lohre’s Cases)

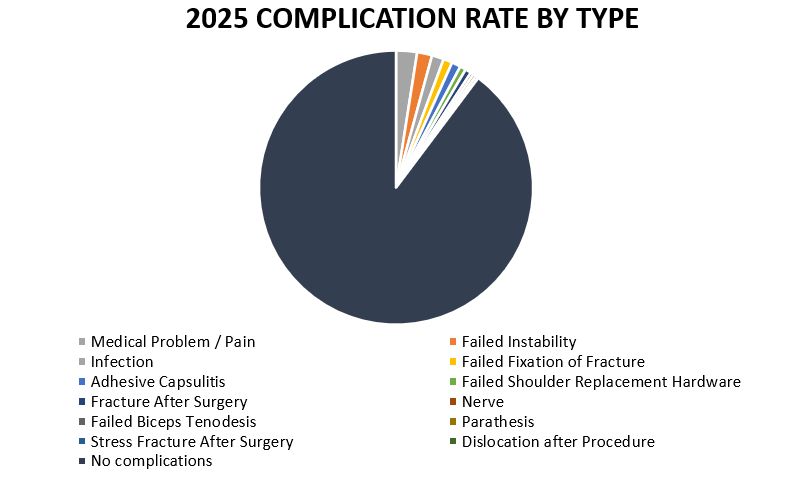
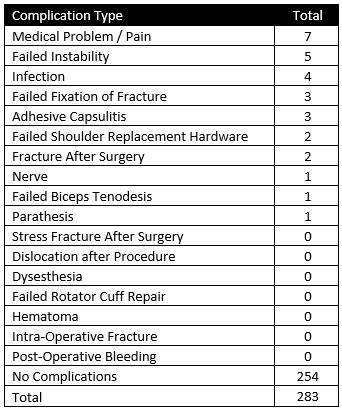
2025 Complications Overview
Of 283 patients operated on by Dr. Lohre in 2025, 29 patients (10.2%) experienced a complication during or after surgery. These complications were identified in 2025. Of the 29 complications, 14 required additional surgeries, 3 have upcoming planned surgery, while the overall re-operation rate was 4.9% (14 reoperations out of 283). An explanation of each complication can be found below. Descriptions in green were patients who had resolution of their complication and those indicated in red have an ongoing issue at the time of this reporting.
Medical Problem / Pain
Patient underwent arthroscopic pectoralis minor release, brachial plexus neurolysis, biceps tenodesis, rotator cuff repair (supraspinatus), and debridement and continued to have significant burning pain similar to before their first and second spine surgery. PT has been difficult and recent MRI showed prior anterior and posterior spinal fusion with interval change of a C4/5 disc. Imaging showed no overt structural causes of pain and normal post-op appearances including an intact rotator cuff repair. Patient has an appointment scheduled with spine services and will revert back after consulting with them; if they do not feel the neck is a potential cause of this pain then will try a suprascapular nerve injection.
Patient underwent removal of hardware, revision RSA, revision non-union ORIF, bone grafting major using allograft proximal humerus, and pectoralis major repair. Patient admitted pain and weakness present ever since surgery and does not feel like they are progressing even with PT. Activities of daily living remain difficult due to ongoing shoulder dysfunction. CT scan shows no significant bridging of the allograft but no osteolysis and retained position. Will follow-up in 2-3 months for repeat evaluation and discuss the possibility of hardware removal.
Patient underwent arthroscopic pectoralis minor release, biceps tenodesis, and debridement. Patient notes continued severe anterior shoulder pain and stiffness; injection into quadrilateral space did not help. Notably, the patient has had prior cervical procedures, and is now referred to a nerve specialist for surgery after improving with intra-articular steroid injection. Additionally, seeing neurosurgery for continued neck and shoulder pain.
Patient underwent arthroscopic anterior latissimus dorsi tendon transfer reconstruction and debridement. Patient notes lateral elbow and anterior shoulder pain that began immediately after surgery. Pain in anterolateral elbow began after the patient no longer needed arm sling 8 weeks postop. There is concern for possible radial nerve entrapment syndrome. However, patient reported that the function of their shoulder has been improving over and elbow pain is getting better. Patient progressing with PT and will follow-up at the year mark.
Patient underwent RSA. Patient noted triggering of the ring finger, likely due to tendon swelling post-surgery. Now, has obtained steroid injection into finger and continuing to work on range of motion. They are doing better.
Patient underwent Latarjet procedure and initially had a healed bone graft, but developed muscle irritation from friction against the screws which likely was causing inflammation and swelling within the joint. Patient recently reported that they will have another surgery to get the screws removed due to the pain and is waiting to have it scheduled.
Patient underwent revision RSA and irrigation & debridement. However, the patient’s post-op course was complicated by pancytopenia for which internal medicine and hematology/oncology services were consulted for. During the initial work-up, the patient has an episode of melena for which the gastroenterology team did an EGD on 1/22 which showed moderate portal hypertensive gastropathy without active bleeding but with contact friability throughout majority of the stomach.
Failed Instability
Patient underwent sternoclavicular joint reconstruction. However, was indicated for revision surgery due to ongoing deformity of the medial clavicle compared to the contralateral with some anterior subluxation and prominence. Patient reports an improvement in shoulder pain; however, experiences significant discomfort during manual activities and has been advised to postpone physical therapy for an additional month.
Patient underwent arthroscopic suprascapular nerve release, pectoralis minor release, conjoint tendon release, coracoid excision, and debridement. Patient experienced shoulder dislocation while working in their yard, which resulted in pain, prompting them to seek immediate medical attention. Orthopedic specialists were consulted but declined to intervene. Patient continuing with home PT and will monitor progress.
Patient underwent removal of hardware, capsular release and rotator cuff mobilization, and RSA. However, patient had a failed prosthesis and felt significant pressure feeling in shoulder in which wound began to drain from the proximal aspect. Patient underwent revision RSA and LTT with allograft bone block and grafting proximal humerus to reconstruct the deficient greater tuberosity, I&D. Now doing very well, no pain, back at work without any issue.
Patient underwent removal of hardware and non-incorporated iliac crest allograft, revision ORIF humeral shaft at allograft/native humeral interface with proximal tibial allograft strut, and radial neurolysis. Patient had increased discomfort in the shoulder post-op, in which examination demonstrated obvious anterior dislocation of the prosthesis clinically. After having revision RSA, they now have no pain and doing well with PT.
Patient underwent arthroscopic suprascapular nerve release, pectoralis minor release, brachial plexus neurolysis, biceps tenodesis, removal of hardware sub-coracoid, and debridement. Patient reported persistent pain and soreness in shoulder, describing unusual instability of bone movement when shifting body weight or attempting to stand. Patient underwent revision to address instability and is doing well. Patient still has popping and pain associated with AC reconstruction, but doing PT at home and was given steroid injection for pain.
Infection
Patient underwent revision arthroscopic debridement and irrigation. However, patient subsequently had two washout procedures 9 days apart, but was readmitted to ED 30 days after second washout due to infection around the joint. Patient then received an open irrigation and debridement and placement of vacuum dressing. At a recent follow up, patient elected to schedule for another surgical intervention due to stiffness, difficulties with physical therapy, and range of motion.
Patient underwent revision RSA and excision of heterotopic bone. Following surgery, had significantly positive C.acnes culture and loose hardware. Patient was recommended to continue with oral antibiotic therapy and work on range of motion, which has been progressing with PT. Patient is generally feeling well despite decreased range of motion and will continue PT on own after finishing sessions.
Patient underwent arthroscopic assisted lower trapezius tendon transfer, rotator cuff repair, and debridement and presented to ED after developing a wound infection along posterior incision at the site of allograft attachment to lower trapezius. Patient then underwent irrigation and debridement. However, patient still with pain after receiving multiple injections into AC joint and has agreed to undergo arthroscopic debridement, capsular release, subacromial balloon spacer, AC joint resection, possible biceps tenodesis due to capsular stiffness, AC joint arthritis, biceps pain and quite significant impingement pain.
Patient underwent pyrocarbon hemiarthroplasty and later developed a superficial wound infection around the prosthetic implant after noticing an area of opening of distal wound with prominent suture abscess. Then, underwent irrigation and debridement. Patient initially did better before experiencing more pain as clinical history and laboratory investigations were concerning for a periprosthetic joint infection of C.acnes. Patient then underwent an additional procedure for shoulder component revision, irrigation and debridement, and implant retention. The shoulder exhibits satisfactory healing progress, with the implant and joint demonstrating stability. However, there is persistent capsular stiffness, likely a consequence of previous infection and subsequent surgery.
Failed Fixation of Fracture
Patient underwent removal of hardware from scapula, revision ORIF left acromion/scapular spine with allograft strut, and deltoid and trapezial muscle repair. Patient complained of feeling a snapping sensation in shoulder, although they had been diligent with recovery and adhering to protocol. Imaging showed a displaced acromion fracture adjacent to the plates and prior non-union site. Patient then underwent an acromion ORIF with bioinductive allograft and is now in sling post-op and progressing well with stable fixation and absence of infection.
Patient underwent ORIF proximal humerus greater tuberosity, open rotator cuff repair, and acromion process reduction and fixation. Patient continued to have pain around the shoulder without trauma; CT scan confirmed a recurrent displaced GT fracture of affected humerus with loose anchors. Patient then underwent a lower trapezius tendon transfer reconstruction using an achilles allograft and major bone graft and open rotator cuff repair. Patient is recovering well and surgical site is healing.
Patient underwent right serratus anterior advancement with bone block for snapping scapula syndrome. Patient later contacted office describing severe pain around scapula without any trauma. Imaging showed dissociated inferior pole bone graft from its insertion site. Local bone transfer did not unite and patient sustained fractured from the scapula, which resulted in another procedure: scapula ORIF, revision serratus advancement, and partial scapulectomy. Patient feels improved from surgery and has had no new complications –the catching and pain is dramatically improved.
Adhesive Capsulitis
Patient underwent arthroscopic circumferential capsular release and debridement. The patient’s shoulder remained abnormally stiff following this arthroscopic procedure, but the stiffness is likely due to an ORIF proximal humerus that the patient underwent in December 2024. The patient had been performing PT and received a cortisone injection, which provided some relief but no improvement in range of motion. Patient no longer participating in PT due to a plateau in progress. The patient elected to trial one more injection at recent follow-up and expressed interest in scheduling another surgery in summer 2026. They will monitor symptoms and reach out to schedule surgery if they persist.
Patient underwent arthroscopic biceps tenodesis, debridement, suprascapular nerve release, and axillary nerve release. Patient developed stiffness / frozen shoulder post-op and reported a significant increase in shoulder pain, which led to two cortisone injections into the glenohumeral joint. Patient now working with PT so will continue to monitor and call back if anything changes.
Patient underwent arthroscopic rotator cuff repair, biceps tenodesis and debridement. Following this, patient remained stiff 3 months post-op and declined a steroid injection, but has continued doing home PT and formal PT about 2x per week.
Failed Shoulder Replacement Hardware
Patient underwent revision RSA, glenoid bone grafting, open release capsular contracture, coracoid osteotomy, open biopsies, and irrigation and debridement. Patient later reported a sensation of instability in shoulder and imaging demonstrated broken screw of glenoid baseplate and possible loosening of baseplate. Patient underwent a re-revision RSA and reports significant improvement in shoulder pain. However, there is slight concern due to immobilization and pain that is expected to resolve with stability. Patient will continue with PT.
Patient underwent RSA and biceps tenodesis. Then, patient had worsening of shoulder pain 8 weeks post-op and imaging confirmed superior inclined baseplate failure. Patient subsequently underwent revision RSA. However, then fell and had recurrent base plate failure and underwent removal of hardware and re-revision RSA to hemiarthroplasty with anterior latissimus dorsi tendon transfer, anterior teres major tendon transfer, and pectoralis major repair and advancement. Now, the patient reports of no major improvement in condition thus far. They have trouble in elevation of arm and notes a clicking sound during certain movements. The patient expresses interest in resuming PT.
Fracture After Surgery
Patient underwent AC joint reconstruction with allograft. Patient then followed up after being hit by a car while riding a bike and later had another fall, resulting in worsening conditions with increased pain. Patient sustained a fracture around prior surgical site. Patient then underwent revision AC joint reconstruction, and later expressed concern about the position of scapula, feeling that it is not where it should be. Patient now scheduled for removal of hardware since plate is causing discomfort, inhibiting normal joint rotation.
Patient underwent RSA. Patient later complained about stiffness and pain, in which a CT scan confirmed a displaced glenoid fracture without failure of the screws/post or implant position relative to this bone nor any apparent loosening. Patient then had a fall resulting in 10/10 pain and was advised to go to the ED in which imaging showed a reduced shoulder. Patient is advised for a revision, but would eventually proceed with surgery once figured out work disposition.
Nerve
Patient underwent RSA, proximal humerus impaction bone grafting, and biceps tenodesis. Then, patient presented with weakness in arm and perception that scapula was mispositioned. It seemed apparent that the patient has had some form of nerve injury. After EMG, condition did not improve and continued to report persistent shoulder discomfort, despite ongoing PT. Patient developed bursitis in elbow following an increase in weight during PT, resulting in a noticeable bone protrusion. Conservative management with compression wraps and avoiding pressure on the elbow was recommended, however, the patient recently underwent a nerve transfer with a nerve specialist.
Failed Biceps Tenodesis
Patient underwent arthroscopic rotator cuff repair, biceps tenodesis, and debridement. Patient found to have some bulging of the biceps secondary to likely loosening of the biceps tenodesis fixation, which shouldn’t not affect overall strength on the shoulder. Patient was offered surgery to correct, which patient deferred, but will let us know if mind changes.
Parathesis
Patient underwent arthroscopic pectoralis minor release, brachial plexus neurolysis, and debridement. Patient then showed signs of proximal compression of the plexus at the level of the scalene triangle with positive Tinel sign and has more distal cubital and carpal tunnel positive Tinel and compression signs. Patient received an EMG test, which did not reflect a dynamic compression of the plexus as in nTOS. A Doppler US confirmed complete occlusion of left veinous system in keeping with TOS. Patient had a scheduled IR guided onabotulinum injection of scalenes which helped with symptom management. Patient is now referred to the TOS program and a cardiothoracic surgeon to discuss further treatment and possible first rib resection.