Suprascapular Neuropathy
(Tim Hartshorn, MD; David Privitera, MD; Paul Yannopoulos, BA; Jon JP Warner, MD) December 2012
This is a condition which is due to irritation to the SSN. It can result in pain, weakness, or both. Typically it is a chronic condition which is relatively rare, and so it is commonly not diagnosed until other more common causes of shoulder pain, such as rotator cuff tear, acromioclavicular joint disease, or cervical spine (neck) disc disease have already been considered. In fact, sometimes patients have surgery for these other conditions but continue to have pain due to unrecognized SSN irritation.
Patients usually feel deep pain over the top and back of the shoulder. Some indviduals note only weakness without pain, such as volleyball players who develop injury to the nerve from constant stretching during their overhead motions during volleyball.

Nerves provide sensation to the joint and surrounding are and also make muscles contract by bringing electrical impulses from the spinal cord. While in the past it was believe the SSN was only responsible for muscle contraction (motor nerve) it is now known that it also provides sensation to the shoulder joint area and carries pain fibers as well.
The SSN comes from the spinal cord which sends nerve branches to the brachial plexus that carries nerves down the arm. The SSN originates above the brachial plexus being made up of branches from the C4, C5, C6 levels that come together to form the SSN. It then runs down into the neck underneath the clavicle bone and into a notch on the top of the scapula. It then goes underneath the muscles of the rotator cuff to which it gives small nerve branches.. The electrical impulses carried in the SSN allows the muscles of the rotator cuff to contract and make the shoulder move.
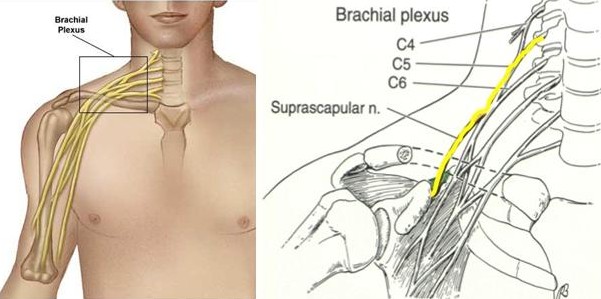
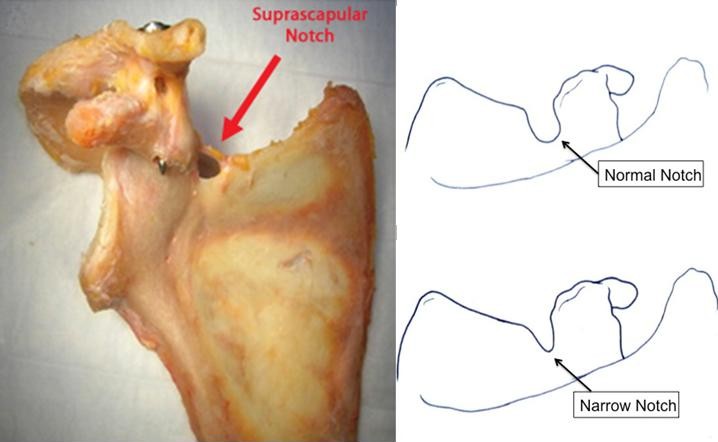
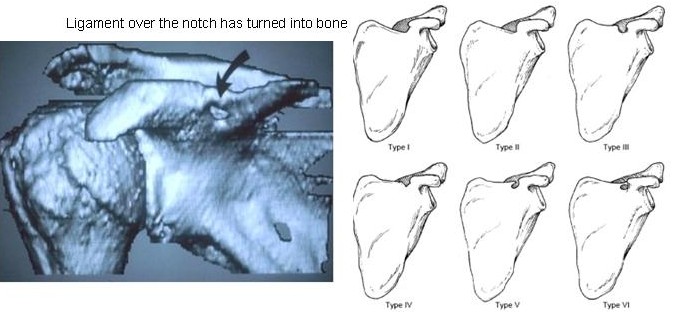
The SSN runs through a narrow opening in the scapula called the Suprascapular notch. This opening is normally wide, but it can be narrow or the ligament over the top of the notch can be solid bone. Both of these variations can predispose the nerve to irritation.
Pain and weakness may occur as the result of several mechanisms.
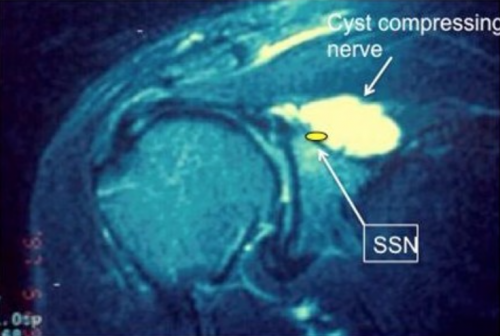
First, the nerve may be compressed by a local mass as it runs through the suprascapular notch and around the scapular spine. A typical cause is a cyst which occurs as the result of a blow-out of the joint capsule. This usually is the result of a tear in the labrum which is the lining of the joint.
The nerve can also be irritated from excessive traction. This can occur due to winging of the scapula. This condition may result from weakness of the muscles which control the scapula or injury to the nerve which makes the scapular muscles work properly.
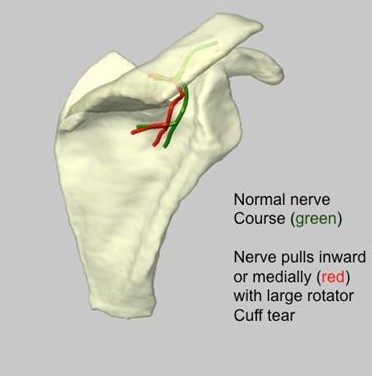
The nerve may also be stretch in the case where there is a large rotator cuff tear. As the tendon tears and pulls away from its normal attachment (retracts) the nerve, which is attached to the muscle, is pulled at an angle and may kink as it goes through the suprascapular notch or around the base of the scapular spine where it is in a fixed position.
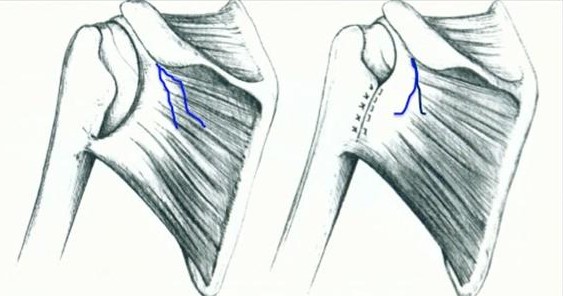
In the figure above, when the tendon tears the nerve is moved away from the joint (left image) and comes under stretch. With repair of the tendon, the nerve is moved back to it’s normal position (above right and below)
SSN is generally believed to be a rare condition; however, it is well known that anesthesizing (numbing) the SSN with an injection can relieve shoulder pain in many conditions. Thus the suprascapular nerve does control pain in the shoulder.
In our recent analysis this condition accounted for 4% of over 1000 new shoulder patients evaluated during a one year period About half of these patients had an associated rotator cuff tendon tear while the other half had no tendon tear.
- Shi LL, Freehill MT, Yannopoulos P, Warner JJ.: Suprascapular nerve: is it important in cuff pathology? Adv Orthop. 2012; 2012: 516985. doi: 10.1155/2012/516985. Epub 2012 Nov 1.
- Freehill MT, Shi LL, Tompson JD, Warner JJ.: Suprascapular neuropathy: diagnosis and management. Phys Sportsmed. 2012 Feb;40(1):72-83.
- Boykin RE, Friedman DJ, Higgins LD, Warner JJ.: Suprascapular neuropathy. J Bone Joint Surg Am. 2010 Oct 6;92(13):2348-64.
Patients with SSN typically have pain over the top of the shoulder and often have weakness of the rotator cuff muscles which includes abduction (raising the arm from the side) and external rotation (bringing the arm out away from the body with the elbow remaining at the side during this motion.). The muscles become weaker due to stretch or compression of the SSN which then does not conduct electrical impulses properly to make the muscle work.
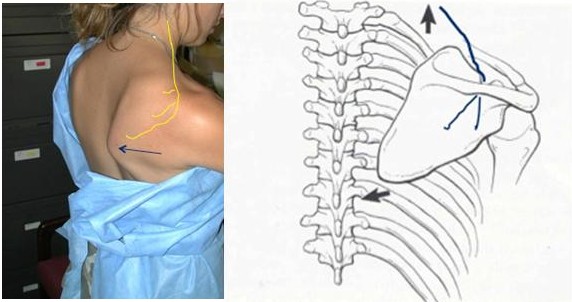
There may also be atrophy of the infraspinatus muscle in the back of the shoulder (see figure) and when this occurs it is usually associated with marked weakness in the setting of a chronic SSN dysfunction.

On the left side there is wasting or atrophy of the infraspinatus (examiner’s hand) compared to the right side where this muscle is more full in appearance.
An Electromyography/Nerve conduction study (EMG/NCV) may be helpful to determine the functioning of the nerve. This is a study done for other common nerve problems such as carpel tunnel syndrome. This study measures the ability of the nerve to conduct electrical impulses by measure the speed and amplitude (size) of the signal as it travels down the nerve. However, this study usually indicates a significant dysfunction of the nerve and in some patients the nerve may be irritated and the EMG study normal if there is no major structural effect on the nerve. In fact publish articles suggest it is only 71-90% accurate in detecting SSN dysfunction. So a negative EMG does not completely rule out a SSN dysfunction.
A fluoroscopic (x-ray)-guided or ultrasound-guided injection into the area of the nerve at the suprascapular notch may confirm irritation of the nerve if it significantly reduces pain, even temporarily. In our experience this seems to be a very sensitive test for pain coming from irritation of the nerve. In fact, in our recent (unpulished) study, 90% of patients who had relief with this injection had a good outcome with surgical release of the nerve.

In this fluoroscopic image, we can see the contrast (black) indicating that the needle is in the suprascapular notch. Once the location is confirmed, the anesthetic and steroid are injected.
An MRI may be helpful not only to rule out an associated tear of the rotator cuff but to check for a ganglion cyst which may be pushing on the nerve. (See figure above). Moreover, in some patients there may be evidence of atrophy of fatty change in the muscle as a consequence of long-standing nerve compression. (See figures below).
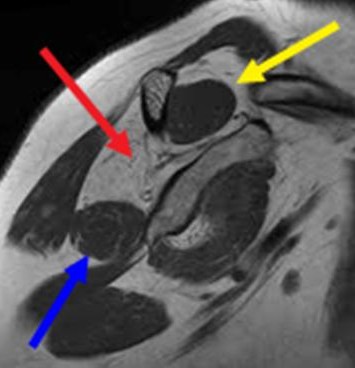
This is a sagittal (cross-sectional) view of the muscles of the rotator cuff. Health muscles of the Supraspinatus (yellow arrow) and teres minor (blue arrow) appear as uniformly gray, while the infraspinatus which is replaced by fat is demonstrated by the red arrow.
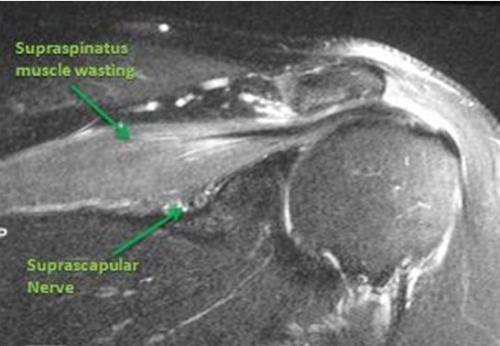
In this coronal (side view) the supraspinatus is shown as lighter due to fatty change and the suprascapular nerve is underneath this muscle
In cases with weakness and without pain, as with a volleyball player who has a stretch injury from overhead sports motion, non-operative treatment is usually the treatment approach. This may include stretching and anti-inflammatory medicatioins.
If there is pain and weakness and the MRI demonstrates a cyst which may be compressing the suprascapular nerve, then a decompression of the cyst and the nerve is a reasonable approach. In such cases, where there is compression of the nerve and weakness, there is a concern that if the nerve is not decompressed it may be damaged and not recover with the result being permanent weakness.
In some patients who have had prior surgery without pain relief, a fluoroscopic injection into the suprascapular notch (as described above) may give pain relief. In such cases, the chronic pain is likely to be relieved by decompression of the nerve.
In patients with large rotator cuff tears who have pain over the top of the shoulder and weakness, if a fluoroscopic-guided injection relieves pain there may be a role for release of the nerve at the time of repair of the rotator cuff. In some of these patients, the tendon may not be reparable, but release of the nerve may give good relief of pain.
In Dr. Warner’s practice the indication for release of the suprascapular nerve is very clear. It is pain relieved by a fluoroscopic-guided injection into the suprascapular notch in patients with and without a rotator cuff tear who have a pattern of pain suggestive of nerve dysfunction.
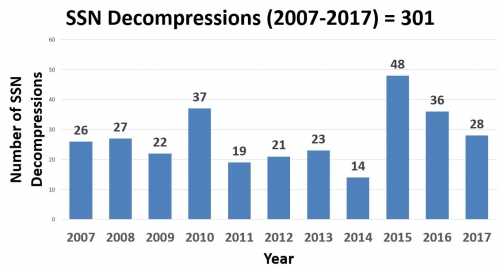
Dr. Warner’s ten-year experience with arthroscopic release of the suprascapular nerve.
Traditionally, the nerve was released at the suprascapular notch using a large incision on the top of the shoulder and removing and then repairing the trapezius muscle (see figures below).
Open Surgery:
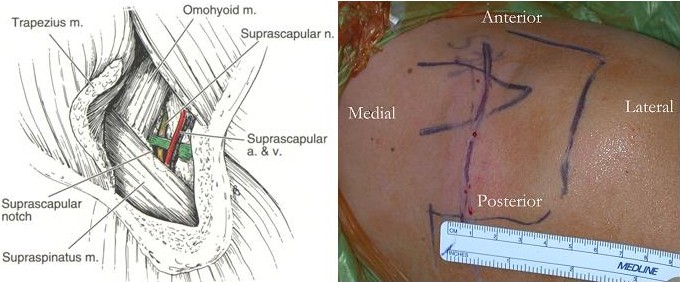
A commonly used approach is a vertical incision over the suprascapular notch. The incision extends from the anterior (front side) shoulder near the clavicle, to the posterior (back side) of the acromion. The trapezius muscle (this muscle allows you to shrug your shoulders) is reflected off the bone of the scapula. The supraspinatus rotator cuff muscle is then retracted away from the nerve and the transverse scapular ligament is then released, while giving caution to preserving both the suprascapular nerve and artery nearby. The trapezius muscle attaches up in the cervical spine and can be uncomfortable for many days to weeks due to its retraction during surgery. Most patients have a significant improvement in their pain and strength. Studies have shown that improvement in infraspinatus (external rotation) strength is less predictable and only about half of patients have improvement in their muscle atrophy. Although the size of the muscle may improve in some patients, the fatty infiltration of the muscle is not expected to change postoperatively.
References:
Fabre T, Piton C, Leclouerec G, Gervais-Delion F, Durandeau A. Entrapment of the suprascapular nerve. J Bone Joint Surg Br. 1999;81:414-9.
Kim DH, Murovic JA, Tiel RL, Kline DG. Management and outcomes of 42 surgical suprascapular nerve injuries and entrapments. Neurosurgery. 2005;57:120-7.
Arthroscopic Decompression of the Suprascapular nerve:
Arthroscopy allows the surgeon to see the nerve and release the ligament over it by making small incisions and looking through a camera. Typically several portals (small incisions) are required (See figure on left below).
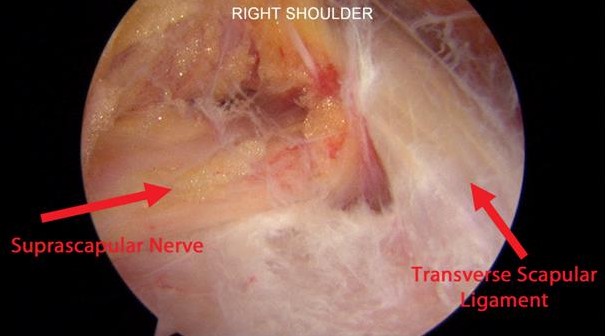
Special arthroscopic portals are used to introduce the arthroscopic instruments so that the suprascapular nerve, artery and transverse scapular ligament are visualized (see pictures below). The nerve can be clearly seen with the arthroscope (images below).

The upper,right image (courtesy of L. Lafosse) shows the nerve (yellow) and the suprascapular artery (red). A cutting device is shown being placed from the portal on the top of the shoulder.
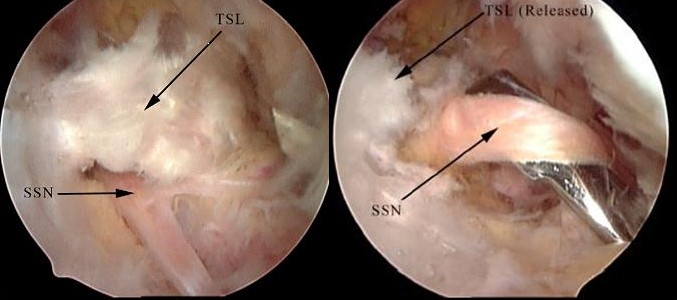
Two lower images: After the nerve and vessel are dissected away from the ligament, the transverse scapular ligament (TSL) is then cut, allowing decompression of the suprascapular nerve (SSN) as seen below. Any related procedures such as a rotator cuff repair can also be arthroscopically performed using this approach.
This image shows the suprascapular nerve running through the suprascapular notch underneath the transverse scapular ligament (which will be released to free up the nerve).
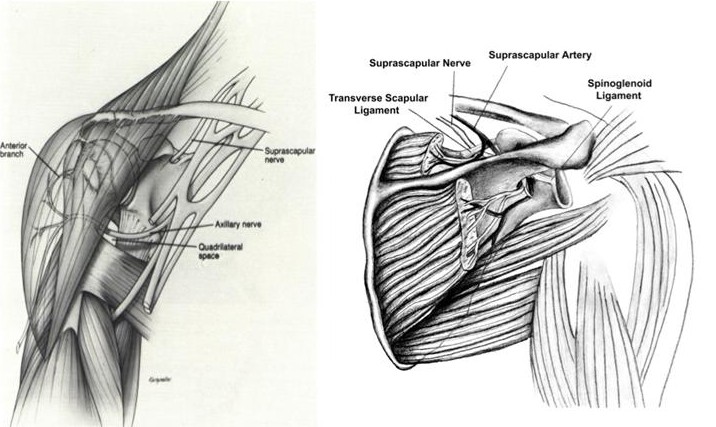
In some patients, the nerve may also be released at the base of the spine of the scapula as it runs down to the infraspinatus. A ligament called the spinoglenoid ligament may also be released (reference Plancher and find image showing this anatomy). Decompression of the nerve may also be required when there is a cyst compressing it at this location (see image above) though repair of the labrum tearn which leads to the cyst may result in decompression of the cyst and relief of pressure on the nerve in over 80% of cases even without nerve decompression.
- Antoniou J, Tae SK, Williams GR, Bird S, Ramsey ML, Iannotti JP. Suprascapular neuropathy. Variability in the diagnosis, treatment, and outcome. Clin Orthop Relat Res. 2001;386:131-8.
- Tung GA, Entzian D, Stern JB, Green A. MR imaging and MR arthrography of paraglenoid labral cysts. AJR Am J Roentgenol. 2000;174:1707-15.
- Piatt BE, Hawkins RJ, Fritz RC, Ho CP, Wolf E, Schickendantz M. Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg. 2002;11:600-4.
- Schroder CP, Skare O, Stiris M, Gjengedal E, Uppheim G, Brox JI. Treatment of labral tears with associated spinoglenoid cysts without cyst decompression. J Bone Joint Surg Am. 2008;90:523-30.
- Chen AL, Ong BC, Rose DJ. Arthroscopic management of spinoglenoid cysts associated with SLAP lesions and suprascapular neuropathy. Arthroscopy. 2003;19:E15-21.
- Lichtenberg S, Magosch P, Habermeyer P. Compression of the suprascapular nerve by a ganglion cyst of the spinoglenoid notch: the arthroscopic solution. Knee Surg Sports Traumatol Arthrosc. 2004;12:72-9.
Several reports have shown a reliable relief of pain and improved strength after decompression of the suprascapular nerve.
Lafosse L, Tomasi A, Corbett S, Baier G, Willems K, Gobezie R.: Arthroscopic release of suprascapular nerve entrapment at the suprascapular notch: technique and preliminary results. Arthroscopy. 2007 Jan;23(1):34-42.
Bhatia DN, de Beer JF, van Rooyen KS, du Toit DF.:.Arthroscopic suprascapular nerve decompression at the suprascapular notch. Arthroscopy. 2006 Sep;22(9):1009-13
We have found very reliable outcome in our patients with arthroscopic release of the nerve giving profound pain relief in 71% within 9 weeks of surgery.
Shah AA, Butler RB, Sung SY, Wells JH, Higgins LD, Warner JJ.: Clinical outcomes of suprascapular nerve decompression. J Shoulder Elbow Surg. 2011 Sep;20(6):975-82. Epub 2011 Feb 1.

42 year old woman 4 months after nerve release with complete pain relief and return to rock climbing.
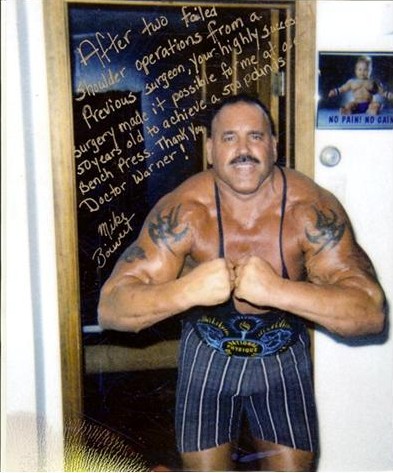
52 year old bodybuilder and weight lifter one year after suprascapular nerve release and partial repair of a massive rotator cuff tear. He achieves his goal of a 500 lb. bench press.