Impingement and Rotator Cuff Injuries
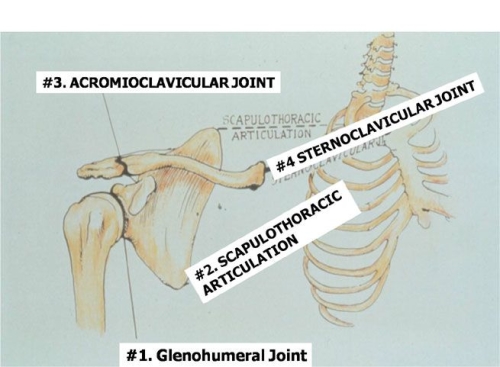
The shoulder is a complex of joints that includes the glenohumeral joint (ball-in-socket), the scapulothoracic joint (wing bone moving on the thorax or chest), the acromioclavicular joint (collar bone attachment to the acromion of the scapula) and the sternoclavicular joint (collar bone attachment to the breast bone).The rotator cuff consists of four muscles that connect from the scapula to the humerus bone and form a cuff around the ball and socket. These muscles help the ball move on the socket, but also compress the ball into the socket to maintain a stable fulcrum for rotation when the shoulder moves.
The four muscles of the rotator cuff are the Supraspinatus (top), Subscapularis (front), Infraspinatus, and Teres minor (back).
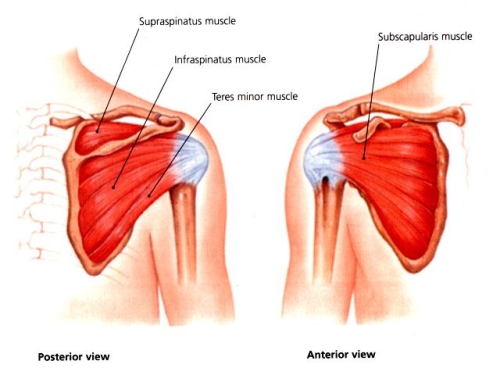
The rotator cuff muscles compress the ball into the socket during active shoulder motion.

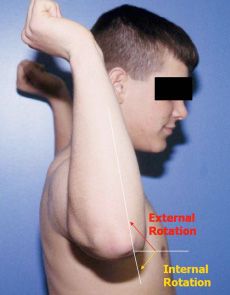
The rotator cuff enables several forms of motion, including flexion (raising your arm over your head), internal rotation (moving the hand inward from the side of the body thus allowing you to put your arm behind your back), and external rotation (moving the hand outward from the side of the body thus allowing you to put your hand behind your head).
Impingement is mechanical compression of the rotator cuff against the acromion bone. This condition may occur with or without the development of a rotator cuff tear. Compression is actually an oversimplification. When the arm is raised with repeated activities such as swimming, tennis, or work, there may be irritation of the bursa, a lubricating tissue layer between the acromion bone and the rotator cuff. If this bursal layer swells due to injury, it may be compressed between the rotator cuff and acromion.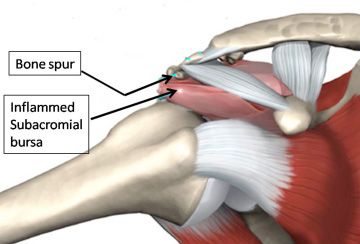
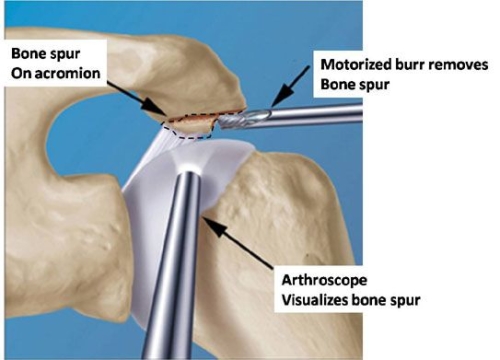
Occasionally, a bone spur may form and contribute to “impingement” or compression of the rotator cuff.
In some patients, a very large bone spur may be an important part of the impingement process, though this is relatively rare. Surgical removal of the bone spur is then performed at the time of shoulder arthroscopy using a special high speed burring device. Removal of the bone spur, along with removal of the inflamed bursa, increases space available for the rotator cuff tendon to move with overhead motions. A new, uninflammed bursa will grow back to replace the inflamed bursa that is surgically removed.
The rotator cuff may be injured from repetitive overhead motion, a sudden trauma, or a combination of the two.During your lifetime, the arm is placed overhead repeatedly, so there is a potential for the rotator cuff tendon to be irritated from compression against the acromion bone.
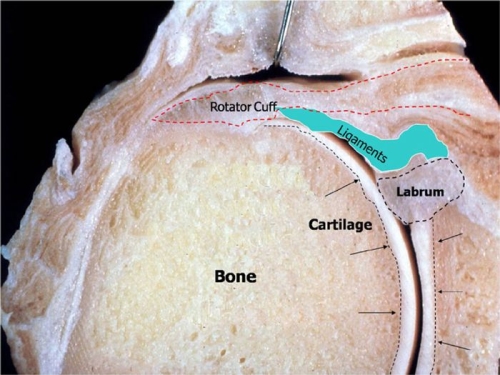
The Rotator cuff attaches on the edge of the humerus bone around the humeral head.
If you have pain, but not much weakness, it is likely that the tendon is irritated but not torn. The lining over the rotator cuff is called the bursa and it may be inflamed as well. This is called a bursitis. The combination of bursitis and irritation of the tendon is called “Impingement Syndrome” (see above).
When the tendon is torn, there will usually be pain, as well as weakness. Another common complaint is night pain that interferes with sleep. The most common tendon that tears is the supraspinatus, the tendon on the top of the ball and socket.
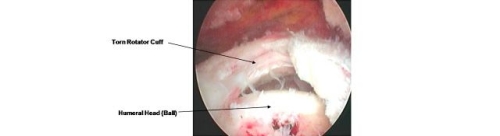
The tear of the supraspinatus tendon is triangular in shape in this image, but it may vary in size and shape.

Arthroscopic appearance of a rotator cuff tear of the supraspinatus tendon.
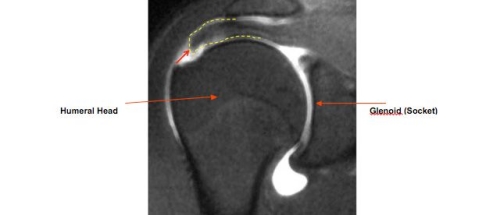
MRI appearance of a tear (red arrow) to the supraspinatus tendon (Yellow broken line).
The rotator cuff may be injured from repetitive overhead motion, a sudden trauma, or a combination of the two.Initial treatment is usually conservative as symptoms may subside over time with the proper therapy program.
Physical Therapy: a program of therapy supervised by a therapist may help improve your strength and reduce your pain.
Anti-inflammatory Medications: Your physician may also prescribe medications to reduce inflammation. These will usually help your pain and facilitate physical therapy.
Cortisone Injection: In some cases, an injection of cortisone may be recommended. This will usually give excellent pain relief. The benefits may include improved ability to sleep at night and improved effectiveness of a physical therapy program. Even if the injection only provides temporary pain relief, it will also help confirm the diagnosis.
Surgery: In most cases, repair of the torn tendon can be performed arthroscopically with the patient going home the same day as the surgery.
Decompression of bone spur causing Impingement on the rotator cuff and removal of inflamed bursa. (See images above under “What is Impingement”)
Repair of a rotator cuff tear by placing sutures through the tendon arthroscopically.
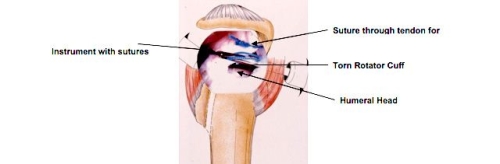
Arthroscopic rotator cuff repair is a common procedure but requires technical skill to not only perform the surgery but make the proper judgement of how to repair the tendon.
Tendons which tear are never normal so the amount of tendon degeneration may vary. Some tendon tears occur in poor, thin tissue Tissue quality is an important factor for tendon healing and success of the repair. In general, chronic longstanding tears have poorer quality tissue and this can be further aggrevated by a history of smoking.
Good quality tendon tissue is characterized by thick tissue with elastic consistency.
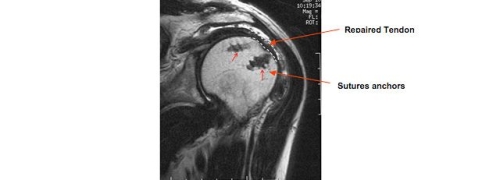
MRI appearance of a healed rotator cuff repair. The suture anchors that have been placed to repair the tendon are shown by red arrows. The healed tendon is outlined in dotted white line.
Recovery from Tendon Repair Surgery: After surgery, the shoulder is usually protected in a sling for 4-6 weeks. A therapy program is then performed under the supervision of a certified physical therapist. Return to sports participation may take 4 months or more from the date of surgery. If there is no need for a tendon repair and only the inflamed bursa and a bone spur is removed, then return to daily use of the arm and sports participation may be on the order of several weeks.
For more information see For Physical Therapists.
QUESTION: How fast will I recover following surgery?
Answer: See our recovery curves on the “How Fast Will I Recover?” page.
QUESTION: Will my tendon heal if I don’t have a surgical repair?
ANSWER: Tendons that tear are not normal to begin with and have undergone some degeneration already. Thus they are weaker than normal tendons. This may be the result of aging, use, and other factors. Tendons that tear do not heal on their own.
QUESTION: Will I have pain if I don’t have a surgical repair?
ANSWER: Pain may resolve, even if the tendon does not heal. Studies have shown, however, that in individuals who use their arms for work or sports tendon repair results in better pain relief and power than nonoperative management.
QUESTION: Will I get worse if I don’t have a surgical repair?
ANSWER: While many individuals may not notice a disability or have pain with a chronic rotator cuff tear, the tendon tear may grow larger over time. Some patients may also become more symptomatic. The risk is that, if the tear gets larger, it may be more difficult to fix in the future. Furthermore, the muscle of the rotator cuff, which is attached to the tendon, may become atrophied (shrink and become smaller). The muscle will also degenerate so that it becomes more fat and scar than actual muscle. If this happens, the rotator cuff muscle will have less potential to contract like a healthy muscle. Repair of the tendon may not be as likely to heal or restore power, once the muscle has atrophied and changed to scar and fat. The time required for such degeneration of the muscle is unknown, but basic studies in animals suggest it may be as fast as 3-6 months after a tendon tear occurs if a traumatic event has been the cause of the tendon tear.
QUESTION: What can I do before surgery to help with healing of my rotator cuff after surgery?
ANSWER: It is well-known that smoking is associated with the development of rotator cuff tears and that such tears tend to be larger in individuals who smoke. Furthermore, it has been shown that cigarette smoke interferes with tendon healing in animals. Thus, if you smoke, you should stop as soon as possible before you have rotator cuff surgery and you should not smoke at all during the recovery.
The use of anti-inflammatory drugs can also interfere with tendon healing, so medications such as aspirin, ibuprofen, advil, and similar drugs should be avoided both before and after shoulder surgery.
QUESTION: How fast will I recover after surgery and when can I play golf? Swing a tennis racket? Run? Weight lift?
ANSWER: Small tendon tears are usually immobilized in a sling for 4 weeks after surgery and larger tears are treated with an initial 6 weeks of sling immobilization. The tendon healing is then strong enough to allow for daily use of the arm, but not sports participation. Strengthening is usually permitted 3 months after surgery and return to skill sports such as golf, tennis and swimming are permitted 4 months after surgery. Weight lifting and collision and contact sports should be avoided for at least 6 months after a rotator cuff repair.
QUESTION: When can I go in the shower after surgery?
ANSWER: It is usually permitted to go in the shower 3 days after surgery as the small incisions required for arthroscopy are sealed over by that time. If there has been a larger incision, as with a biceps tendon tenodesis, your surgeon may advise you to avoid getting the dressing wet. The shower head, in this case, should be angled away from the shoulder.
QUESTION: How good will my shoulder be after surgery?
ANSWER: All patients differ in terms of the quality of the tendon tissue being repaired and the size of the tendon tear. In general, most patients note marked improvement in their pain and improved overall function. Overall, more than 90% of patients feel they benefited from their surgery when asked one year after the surgery. The degree to which strength and power return depends mostly on the quality of the tendon tissue and the completeness of healing of the tendon. Furthermore, the chronicity of the problem may affect the ultimate potential for the rotator cuff muscles to create a powerful shoulder.
QUESTION: What is the risk I might be worse after surgery?
ANSWER:
The complication rate after an arthroscopic rotator cuff repair is low. Possible complications related to anesthesia may include numbness, tingling, pain, and weakness after a nerve block, though these risks are well below 1%. It is extremely rare to have a reaction to anesthesia medications.
Surgical complications may include infection (<1%), bleeding and nerve injury (0% in last 2 years), and shoulder stiffness (<1%). Shoulder stiffness is called “frozen shoulder” and it may actually occur after any surgery on the shoulder. The reason for a frozen shoulder is usually the body over-reacting to the stimulus of surgery and making inflammation and then scarring. This problem typically resolves with a therapy program but the overall recovery may take longer than if the problem does not occur.
On rare occasions a patient may have more pain or less function or both after surgery, despite no clear indication why this may be the case. This may be due to subtle changes in mechanics of shoulder function after surgery. Such an occurrence is well below 1% in our experience.
QUESTION: What kind of anesthesia do you use?
ANSWER:
The anesthesiologist will discuss options with you. Most patients elect to have an interscalene nerve block, a local anesthesia in which the arm and shoulder are made numb. You are also put to sleep using a special mask (LMA= Laryngotracheal mask) is placed over your mouth in order to help you breath. A breathing tube is not usually required with a nerve block.
For more information please go to the Ambulatory Surgery Center Website: http://www2.massgeneral.org/ortho/ASCRegionalAnesthesia.htm
The pain relief with an interscalene nerve block may last well into the evening and this means you may need less pain medication immediately after surgery than if the nerve block was not performed.
If there is some medical reason that you are not a candidate for a nerve block, then general anesthesia is utilized.
QUESTION: Do you ever need to do an open rotator cuff repair or can you do all of these repairs arthroscopically?
ANSWER: Most rotator cuff tears can be fixed arthroscopically. Indications for open surgery are usually related to the need to treat other factors that may result from a previous failed surgery or an associated injury not managed well by an arthroscopic approach. Such factors are deltoid muscle injury, fracture of the acromion bone, and chronic dislocation of the shoulder.
Click Here to view patient testimonials for rotator cuff repair.